LATITUDE & THE INCIDENCE OF DISEASE:
OVERWHELMING PROOF THAT
VITAMIN D3 DEFICIENCY
CAUSES
MOST HUMAN DISEASES
(Please note-. If you feel you have benefited from the information (AND YOU WILL), please hit the share on Facebook/Twitter/Pininterest/LinkedIn buttons at the begining and /or end of this article. And spread the word)
It has been almost six years since I published what was to become the best-selling book about Vitamin D3 in the world – translated into 10 languages so far. I thought I knew everything about Vitamin D3 back when the book was first published because in preparing for writing the book, I read or reviewed all 52,000 abstracts of science journal articles in the Pub Med science database that mentioned Vitamin D.
However, in the last six years I have come up with a simple tactic to see if a disease is caused by Vitamin D3 deficiency and might be treatable with high-dose Vitamin D3. (I have heard from more than 1,000 people using high-dose Vitamin D3 to treat their various illnesses over the years, and have found that high-dose D3 is almost a miracle cure for up to 70 different diseases and conditions, including MS, lupus, depression, Crohn’s disease, psoriasis, and many, many, more!) Of course, if you are new to Vitamin D3 your initial instinct would be to say:
“HA! If it sounds too good to be true – it probably is”.
I assure you this is an exception to that rule as you will soon see and agree.
I will shortly give you MOUNTAINS of overwhelming proof that is really very amazing to consider, but first let me tell you how and why Vitamin D3 can have such miraculous effects on our health.
First of all, Vitamin D3 is not a vitamin!
It is actually a POWERFUL HORMONE that your body makes when sun hits your unprotected skin. It controls or affects over 2,700+ genes in your DNA which are mostly involved with immune system modulation and tissue remodeling- you could say that it is the ultimate biologic. As opposed to biologic drugs that just tweak one section of your immune system to either rev it up or tamp it down, Vitamin D3 tweaks all sections of your immune system at the same time without the dangerous side effects of biologics. Not only does it allow your immune system to “see” good tissues better, thus eliminating all autoimmune attacks, it also revs up the “killer” part of your immune ssytem to attack infections from bacteria, fungi, and viruses as well as newly formed cancer cells.
D3 is a hormone that tells your body that winter is over and summer is here and your body can stop hibernating and can go ahead and repair any incompletely repaired issues you have using all the resources. Most of us humans find ourselves in a state with chronically low Vitamin D3 levels all year long due to sun avoidance and use of sunscreen. I called this state – the Human Hibernation Syndrome. It is when your body acts as if it is preparing for a long winter famine, conserving resources required for repair, slowing your metabolism, and urging you to conserve energy until the winter famine is over.
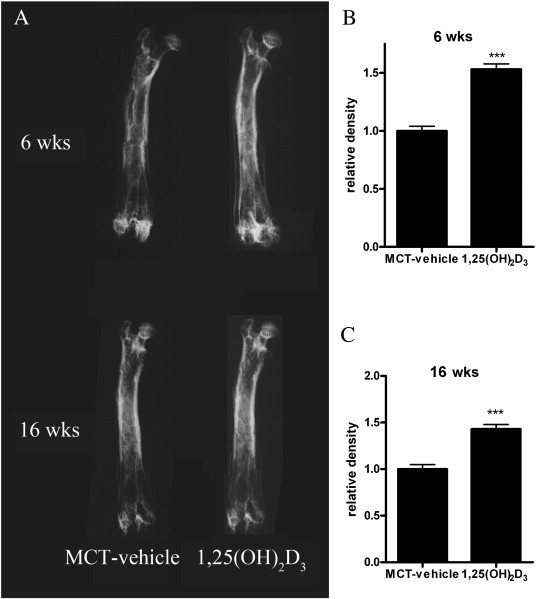
Vitamin D3 is referred to by some researchers as the bone and joint remodeling hormone, and given that I have found how many people also notice its ability to repair the skin and soft tissues; I prefer to call it the all-tissue remodeling hormone.
One of my favorite examples of what Vitamin D3 can do comes in the form of a study they did on some rats. One group of rats received Vitamin D3 in their food while the other group did not. They then broke the poor rats’ legs and then observed how they healed. The rats on a normal diet had healed legs where there was a large glob of extra bone around the break, like it was held together by a big ball of clay. The rats getting Vitamin D3 had perfectly healed fractures and you could not even notice where the break had been! This study says it all – what D3 can do for rat bones it can do for virtually any tissue in your body.
The following illustration is not from the study noted but it gives you an idea:
Basically, your body knows what shape it is supposed to be in. There is an exact blueprint of your entire body located in the DNA in the nucleus of each cell in your body. If your body has a chronic issue or incomplete repair, it is not an accident or loss of blueprint information. It just means your body is waiting until it gets the signal that conditions are right to do the repairs properly. That signal comes in the form of Vitamin D3.
That condition is when summer returns and your Vitamin D3 levels go up and tell your body to go ahead and undo any partial repairs and to redo all the repairs perfectly using all resources necessary.
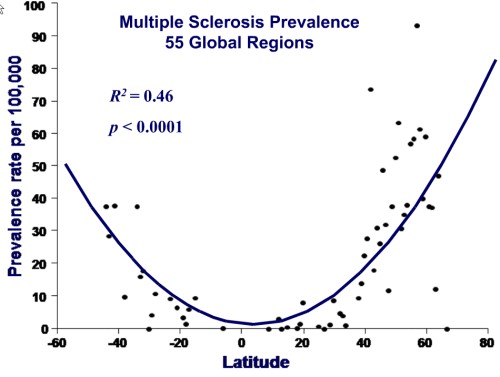
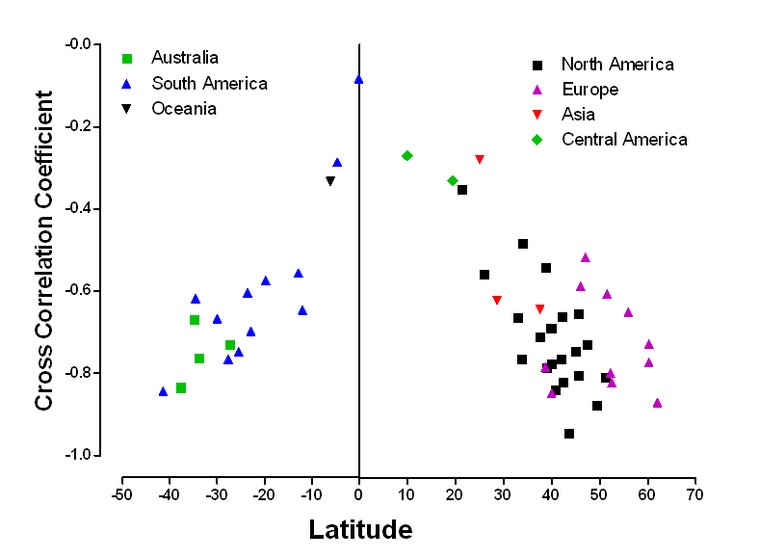
So that’s it, now let’s heap the overwhelming proof on you that is so easy to see. I will simply google-search a long list of diseases, along with the search term latitude, view the google images, and see if there are illustrations showing the incidence of a particular disease that varies in incidence with latitude. If the disease is found at lower rates near the equator and increases as you move away into latitudes with weaker sun, you can bet that it is a Vitamin D3 deficiency related disease
Let’s start with Multiple Sclerosis (my next case study article will be about the 1,000’s of people all over the world who are curing their MS with high-dose Vitamin D3) Here is a graph from a study:
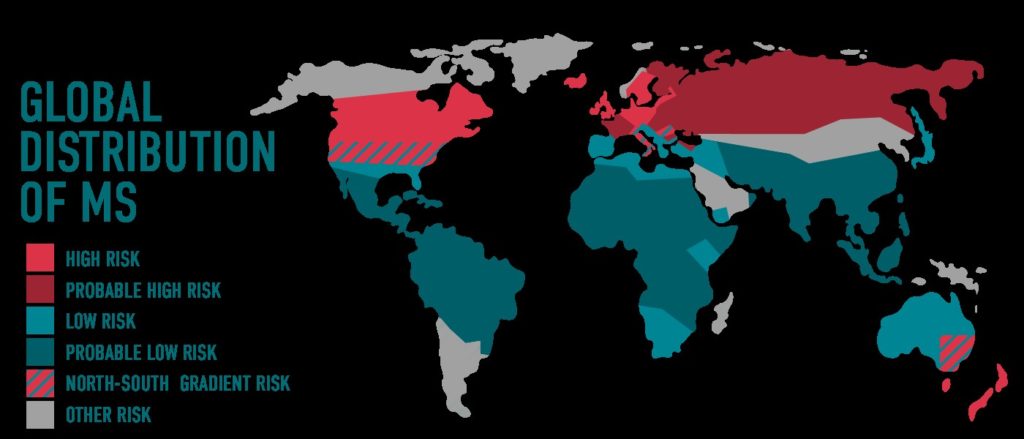
Or another way to look at it:
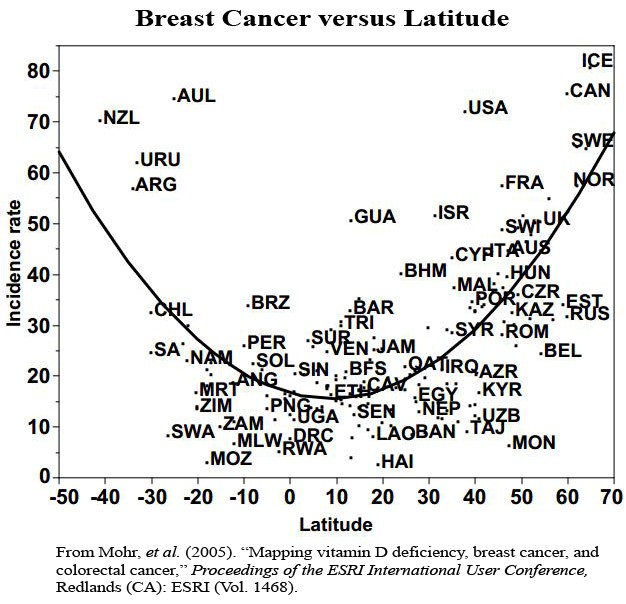
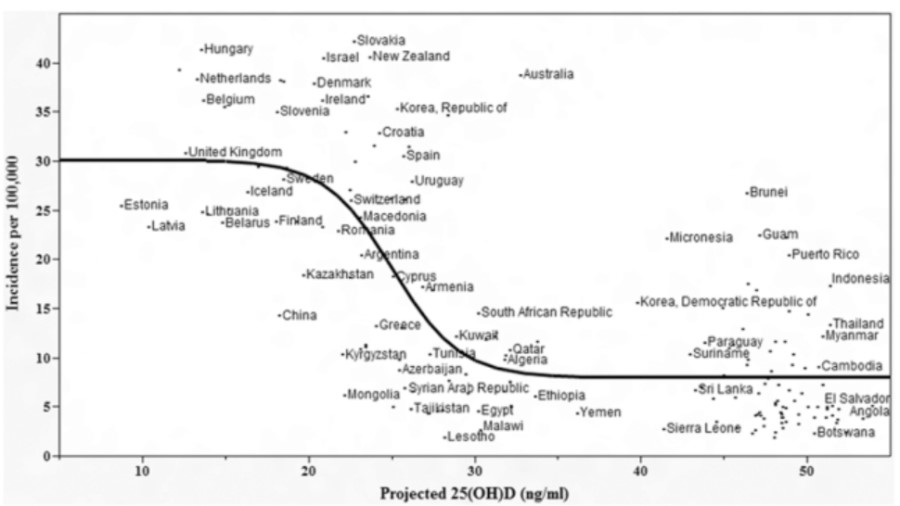
Let’s try breast cancer:
(Oddly- the 23.4 degree (North) circle of latitude around the world is called the Tropic of Cancer, and you will see at latitudes north of 23.4N have much higher cancer rates than south of it! – Now that’s quite a coincidence).
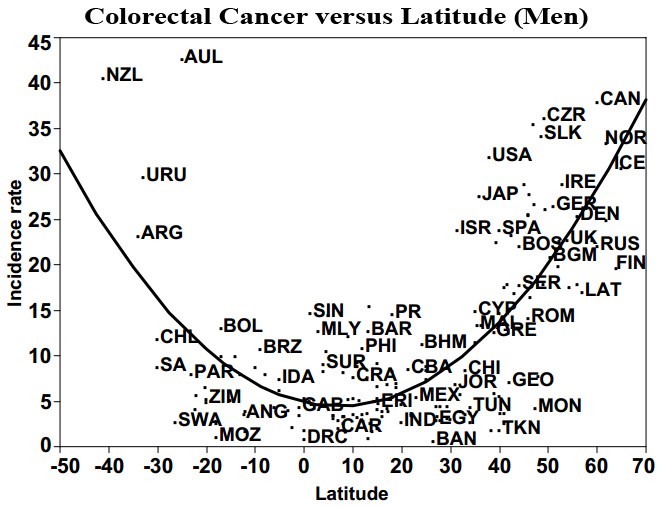
How about Colon Cancer?
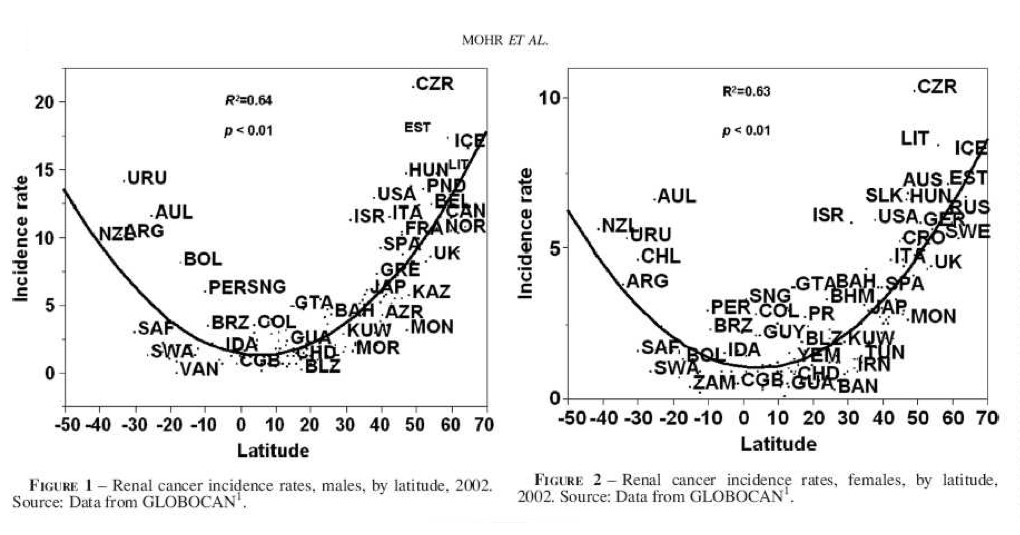
Kidney Cancer:
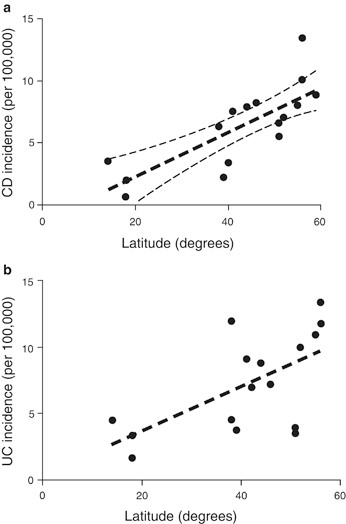
Let’s look at Crohn’s Disease and Ulcerative Colitis:
Psoriasis?
Lupus in the UK:
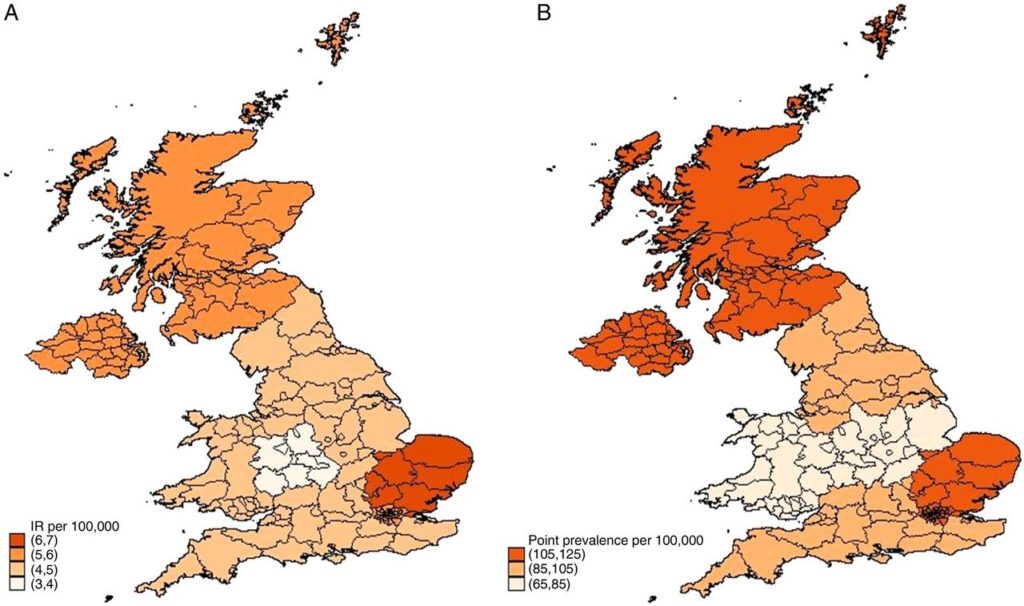
(When you see an anomaly of a high prevalence area where low incidence should be expected, it often is caused by a larger proportion of dark-skinned individuals living in that area. Because it takes a lot more sun in darker skinned individuals to make Vitamin D3 than in lighter skinned ones).
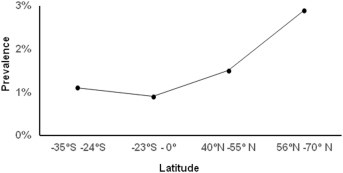
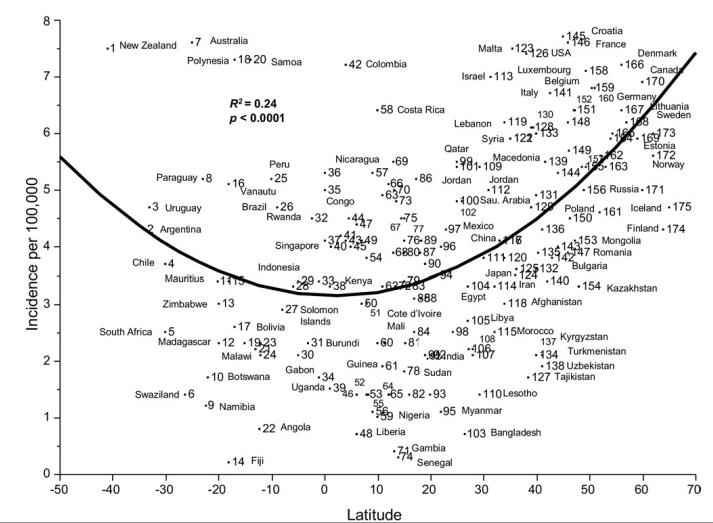
Diabetes (Type 1-Juvenile):
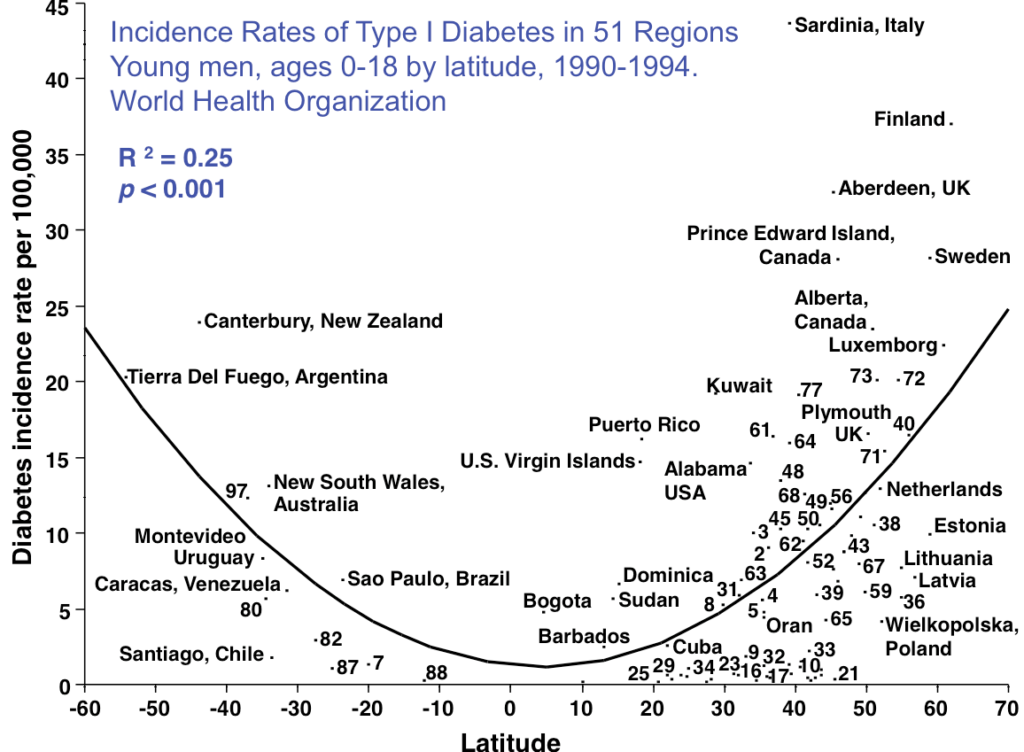
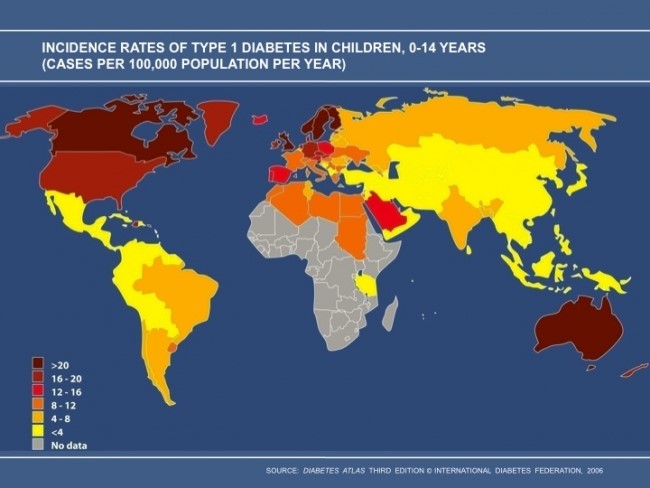
Diabetes (Type 1-Juvenile) cont’d
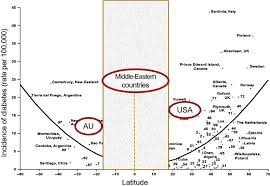
(Keep in mind that sun avoidance is like a religion in the Middle East).
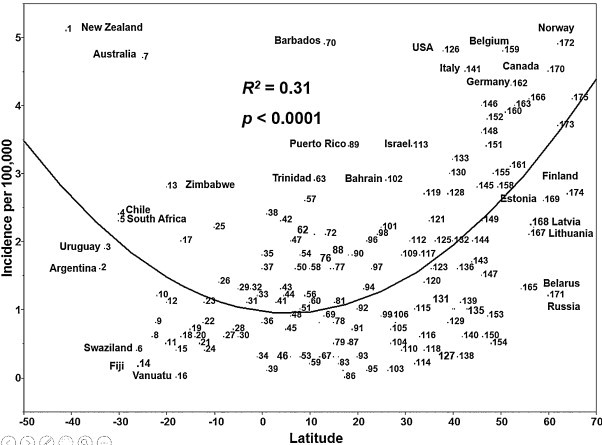
Leukemia vs Latitude:
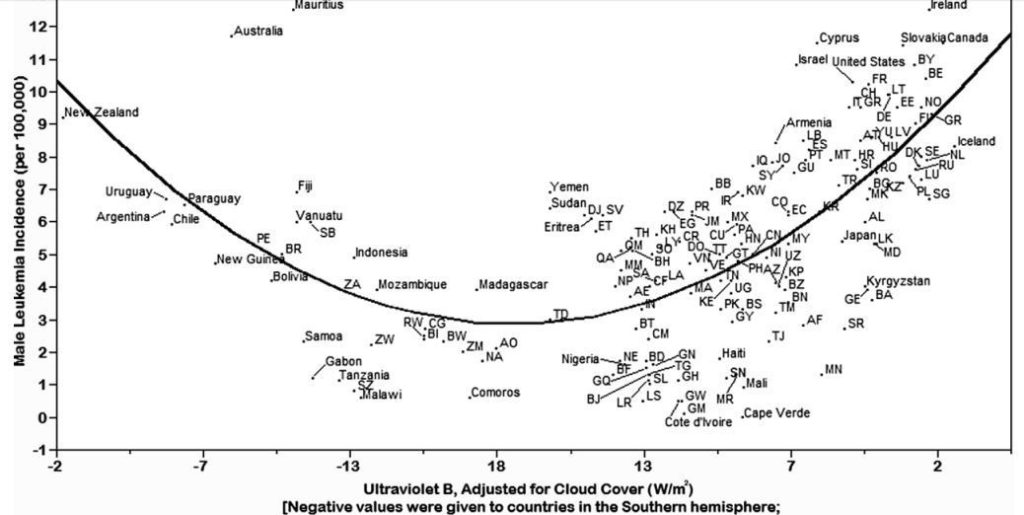
Leukemia vs Cloud Cover:
Multiple Myeloma:
Overall Cancer Rates vs Latitude:
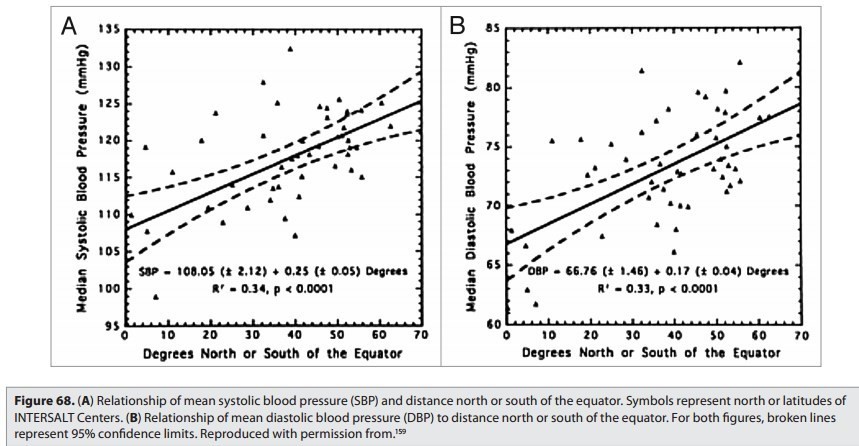
Hypertension:
Tuberculosis:
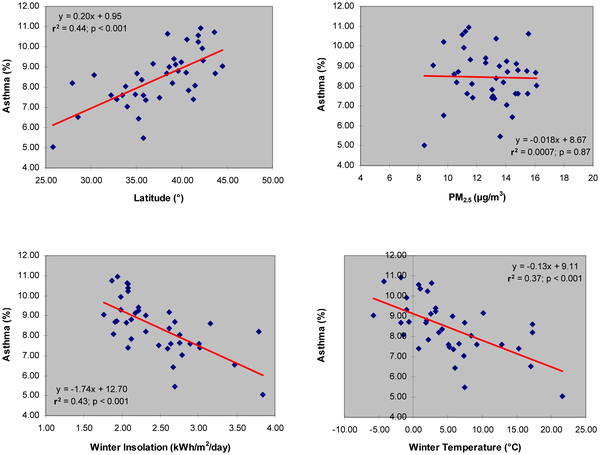
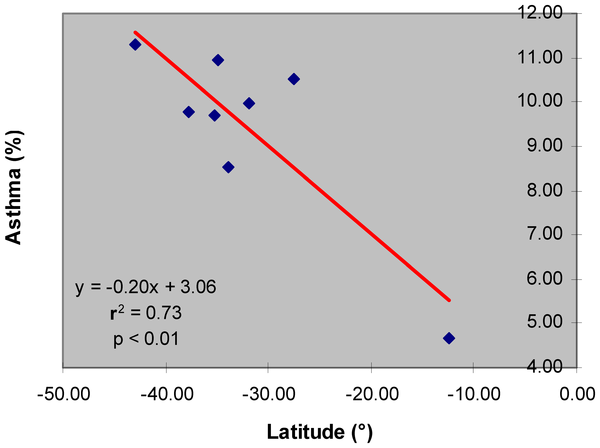
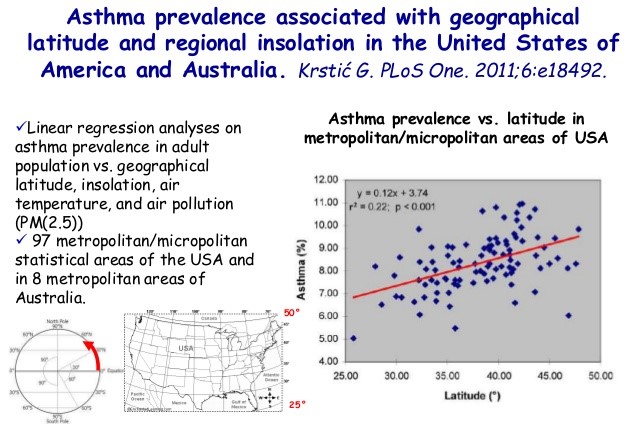
Asthma:
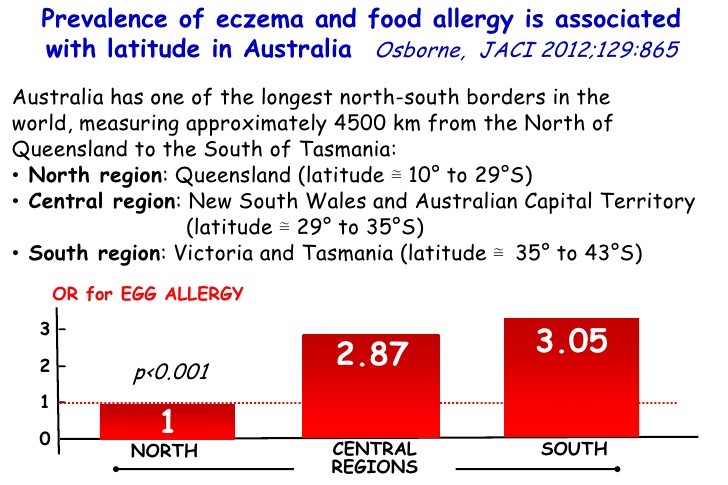
Allergies:
Depression & Suicide:
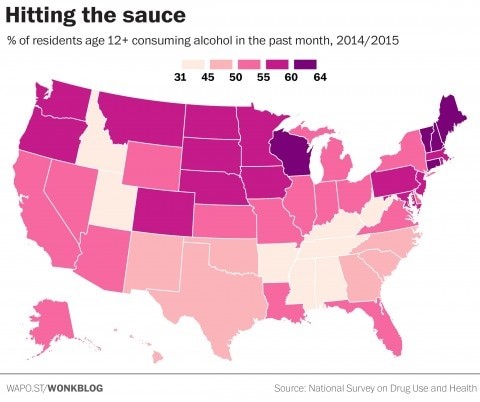
Alcoholism:
Schizophrenia:
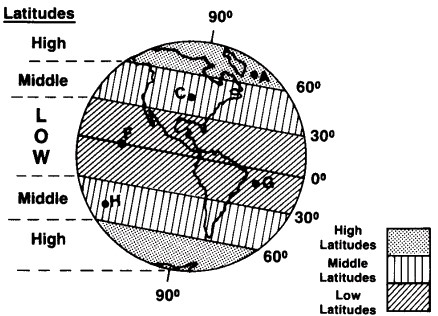
Where are people affected?
So where in the world are there more people in a population living with schizophrenia? The answer comes from a research team who has written multiple papers on the different environmental risk factors for schizophrenia. The study took data from 162 research projects and looked at the incidence and prevalence of schizophrenia within low (equator to 30 degrees), medium (30 to 60 degrees), and high (above 60 degrees) latitudes. While there was little variation found between these latitude ranges for females, there was a significant increase of incidence and prevalence of schizophrenia for males the higher the latitude is.
There have been studies that show people with schizophrenia tend to be born during the winter/spring months. There are also theories that say there could be a correlation between the amount of vitamin D a pregnant woman has during the pregnancy of a fetus who then goes on to develop schizophrenia.
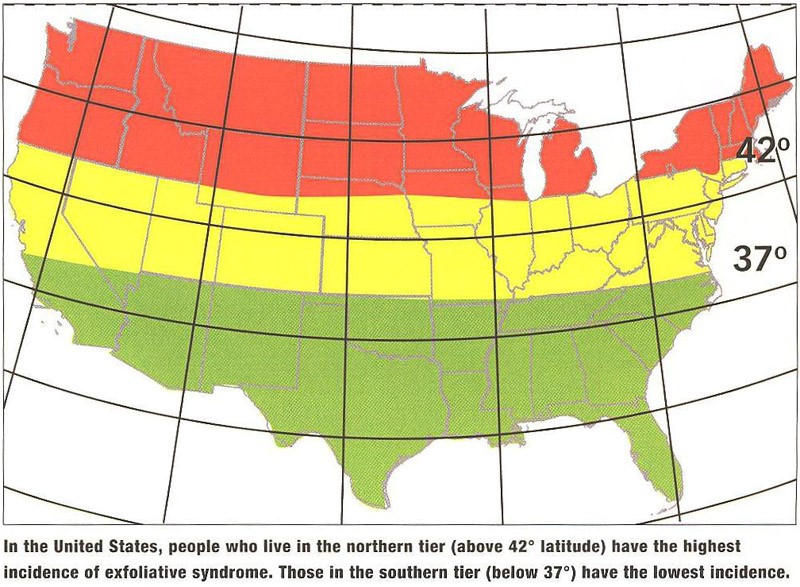
Glaucoma in the US (caused by exfoliative syndrome):
Autism:
A review of prevalence studies of Autism Spectrum Disorder by latitude and solar irradiance impact
Author links open overlay panel Somayya Syeda Kathleen A.Mooreab EvitaM archa
https://doi.org/10.1016/j.mehy.2017.09.012Get rights and content
Abstract
Autism Spectrum Disorder (ASD) is a lifelong disability with no known cause or cure. Among the suggested etiologies, is Cannell’s hypothesis of a deficiency in Vitamin D the main natural source of which is Solar Ultraviolet-B (UVB) radiation. The aim in this paper is to build on this hypothesis and explore the relationship of solar irradiance of which UVB is a component, by latitude with the prevalence rates of ASD. Twenty-five reports published between 2011 and 2016 using comparable diagnostic criteria were reviewed. The results suggest a tendency for the prevalence rates of ASD to be lowest in countries near the equator and for this rate to increase as the latitude increases. These findings provide some support not just for the Vitamin D hypothesis, but also for a new proposition that along with UVB radiation, the entire solar radiation spectrum which reaches the earth, may play a role in ASD. While these results are both novel and encouraging in terms of the potential efficacy of exposure to natural sunlight, further research is warranted before results can be considered definitive, and before the implications of the findings can be implemented clinically.
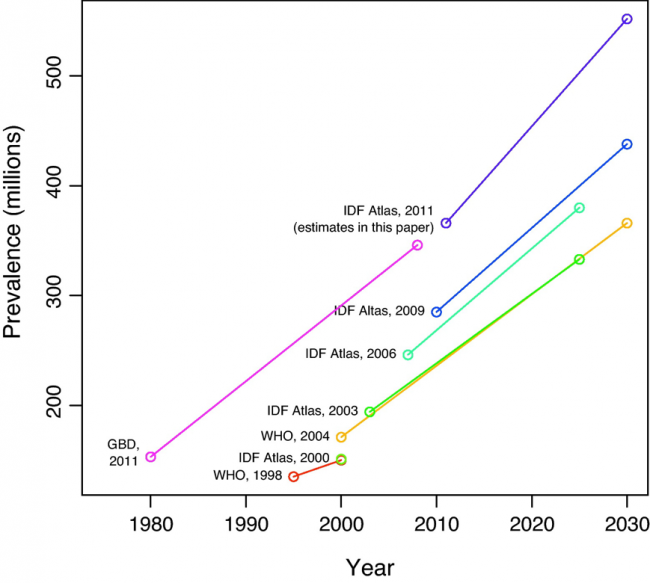
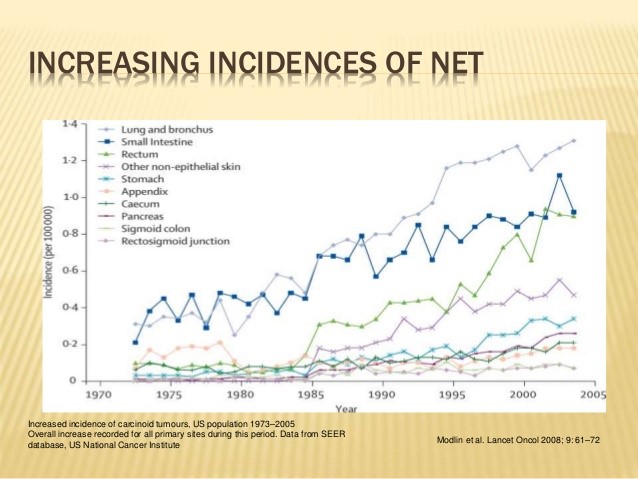
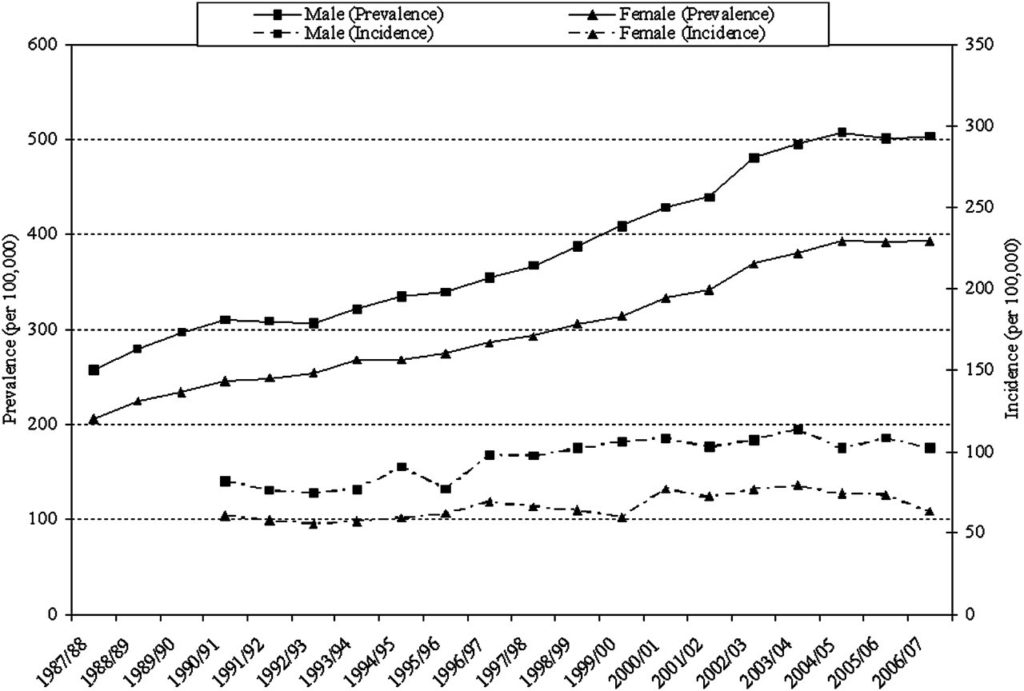
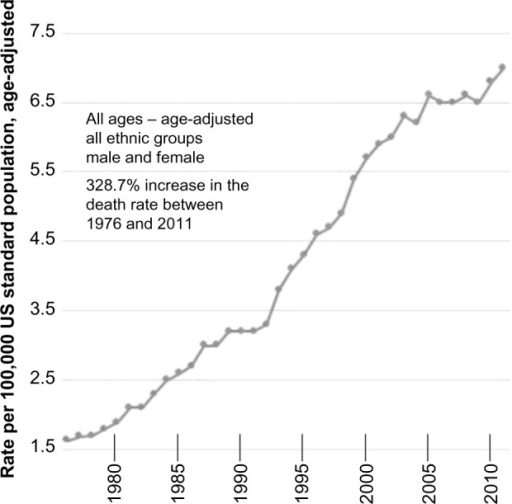
In addition to the latitude effect, we have an
INCREASING PREVALENCE SINCE 1980 EFFECT!
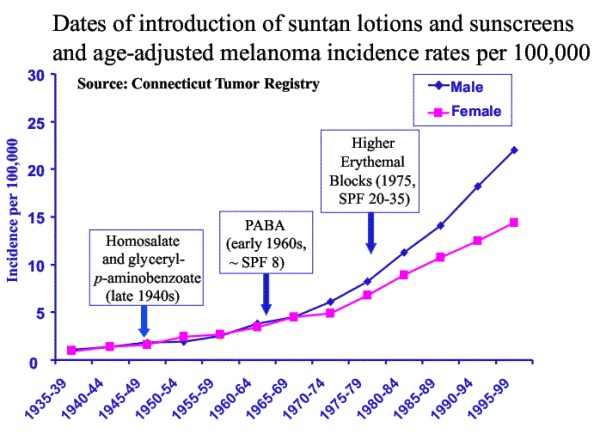
What happened around 1980?
Many more of us started using sunscreen and using more powerful sunscreens while also avoiding the sun:
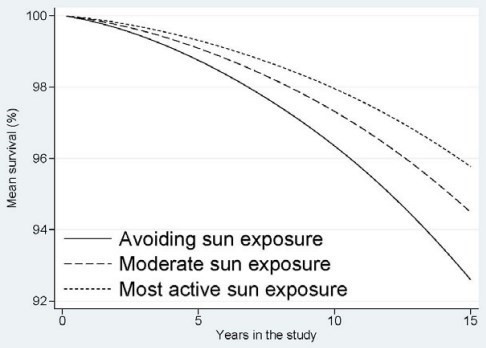
Sun avoidance is associated with earlier death:
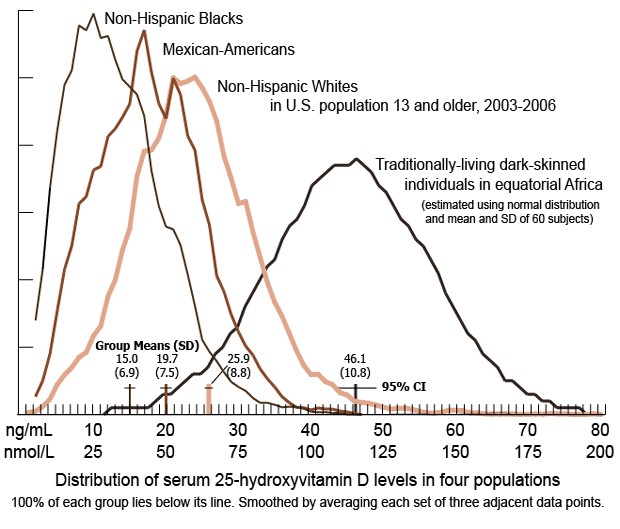
Darker skinned people need more and stronger sun to make the same amount of Vitamin D3 as lighter skinned people in the Northern latitudes – explaining the higher incidence of many diseases seen in darker skinned people living away from the equator.
All of this sunscreen use and sun avoidance since at least the 1980’s has led to an explosive rise in many diseases as you will see in the illustrations that follow:
Cancer:
Bi-polar Disease:
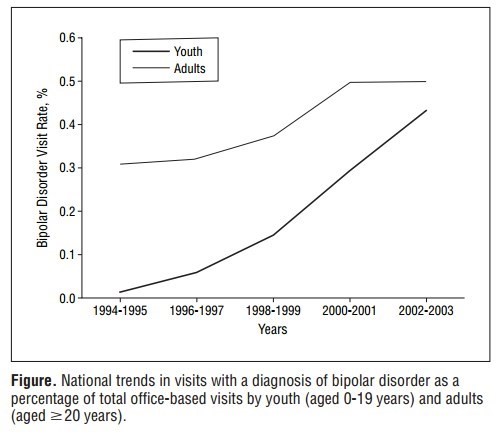
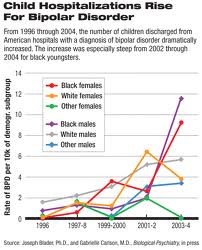
Bi-polar as a % of all youth admissions: 0.01% (1994-1995), 0.44% (2002-2003
From Bipolar Disorder In Children–A Diagnosis in the Doghouse April 2012
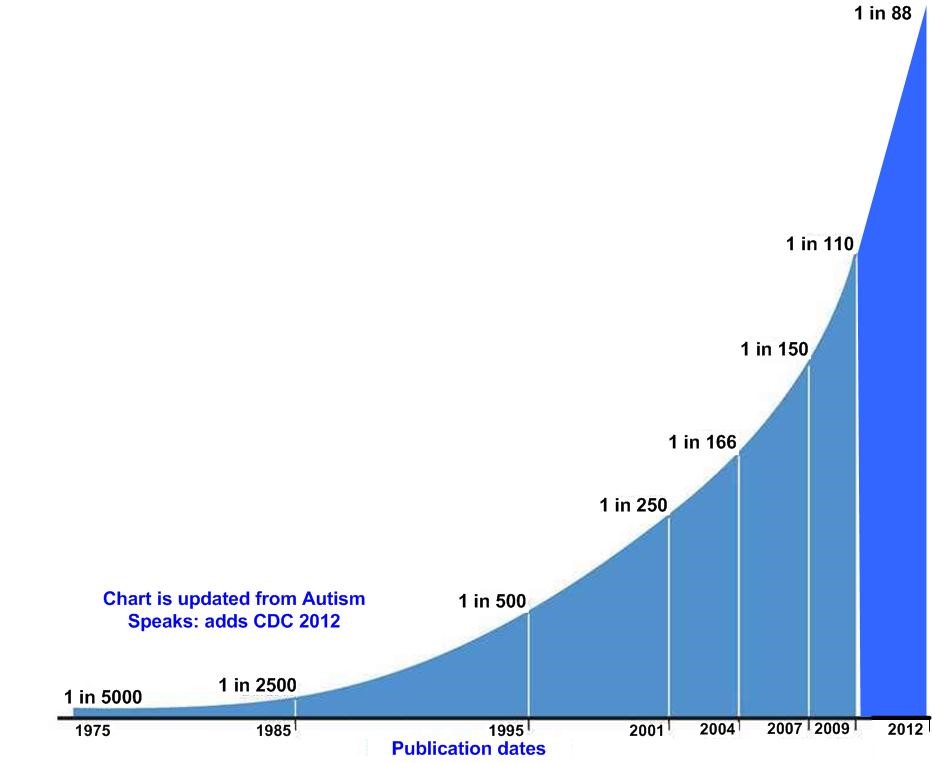
Autism rates have EXPLODED!
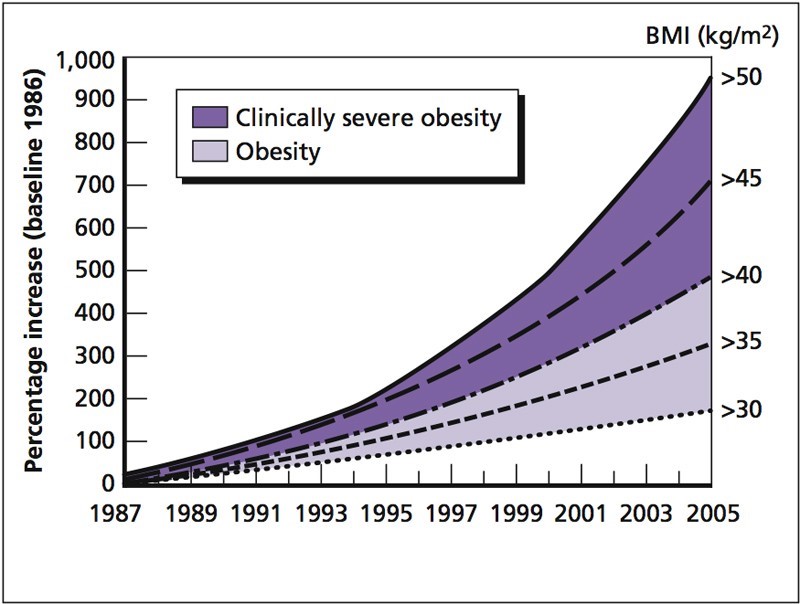
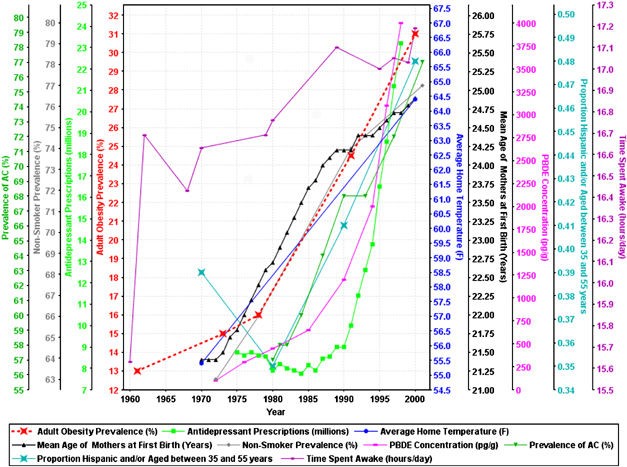
The Obesity Epidemic!
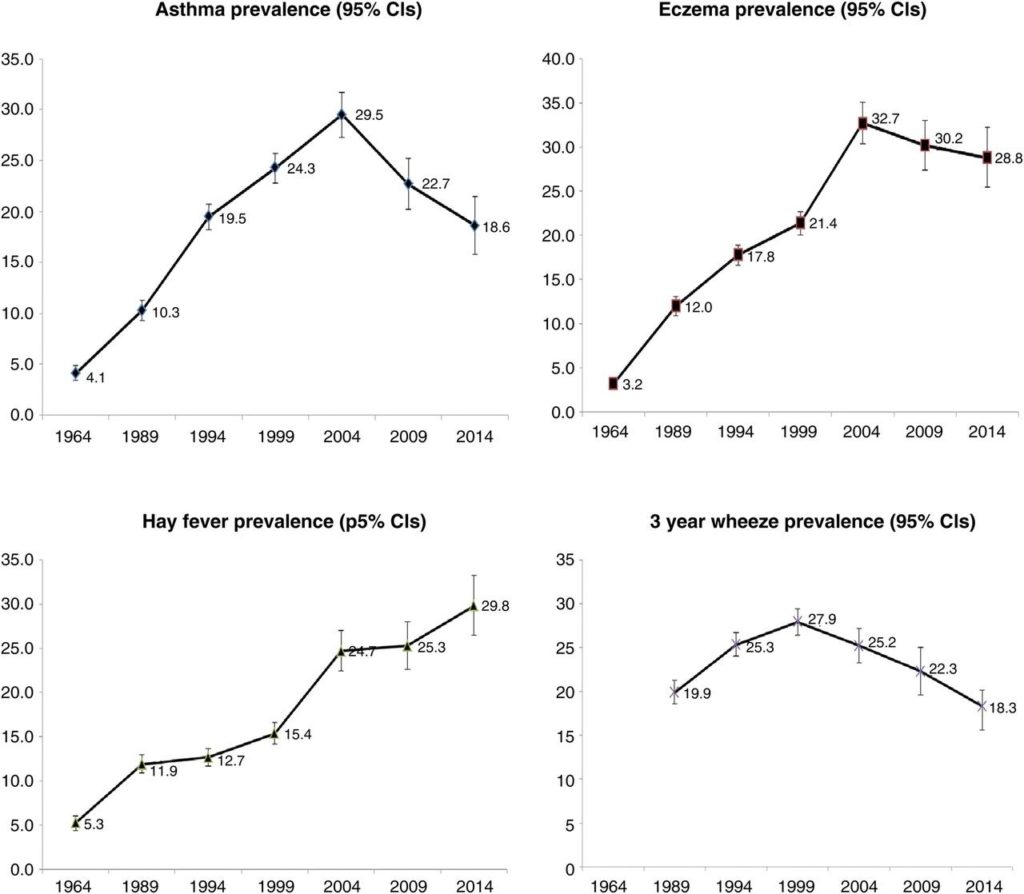
Asthma, Eczema, and Allergies:
Food & Peanut Allergies:
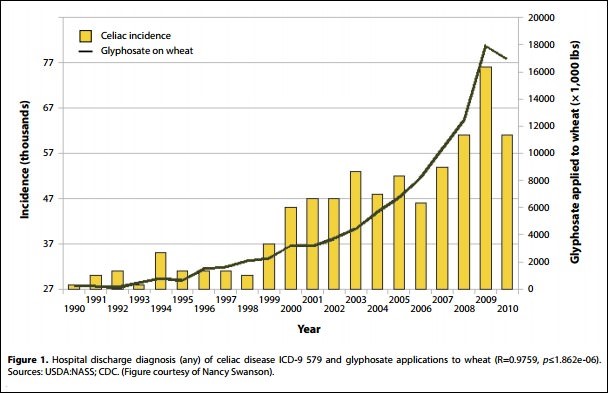
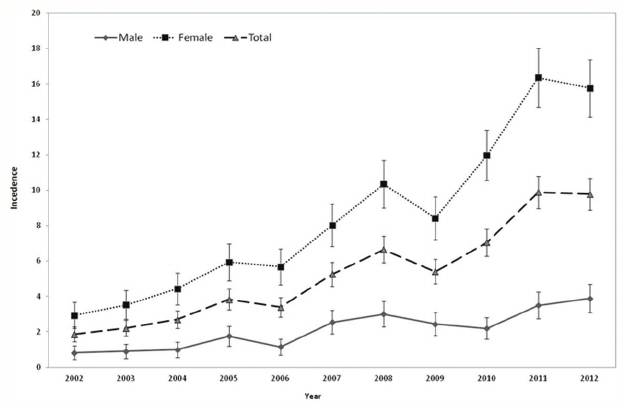
Celiac Disease (Gluten Intolerance):
Multiple Sclerosis is increasing:
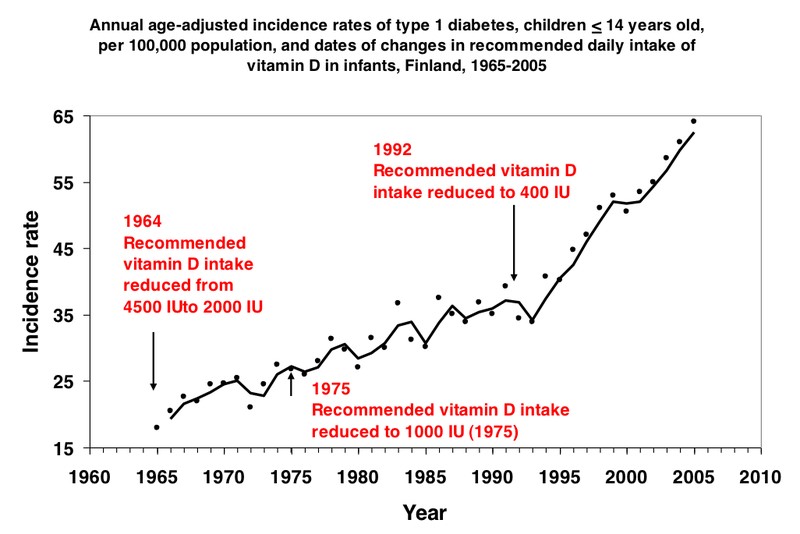
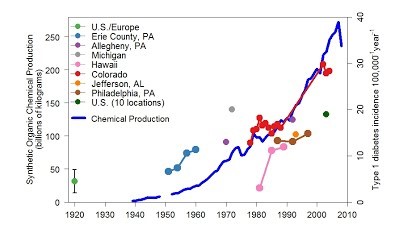
Type 1 (Juvenile) Diabetes:
Type II (Adult) Diabetes:
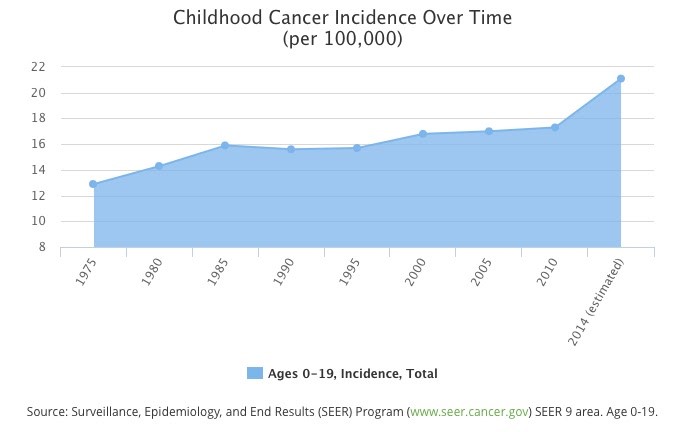
Childhood Cancer:
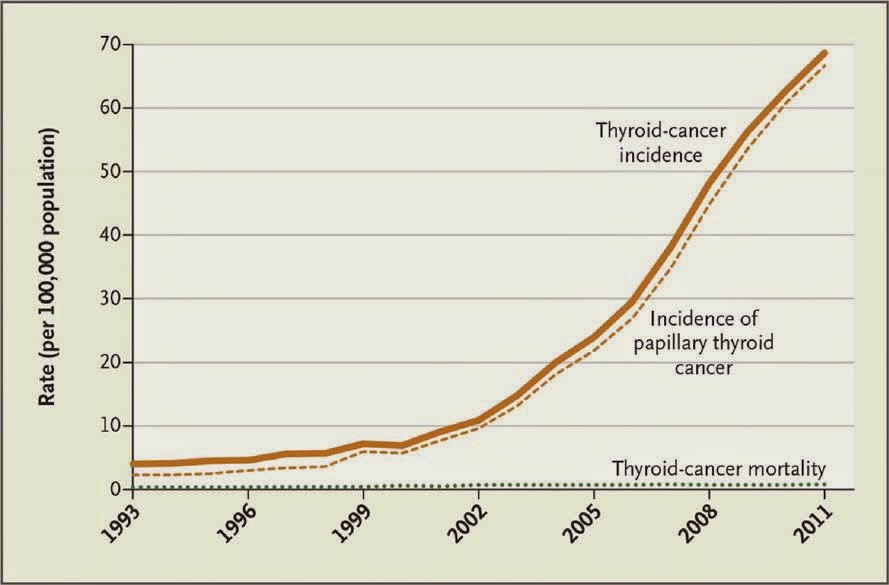
Thyroid Cancer – Exploding!
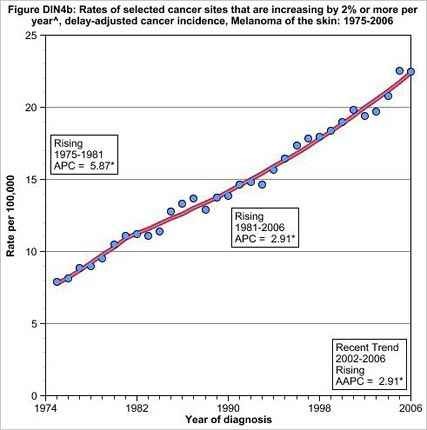
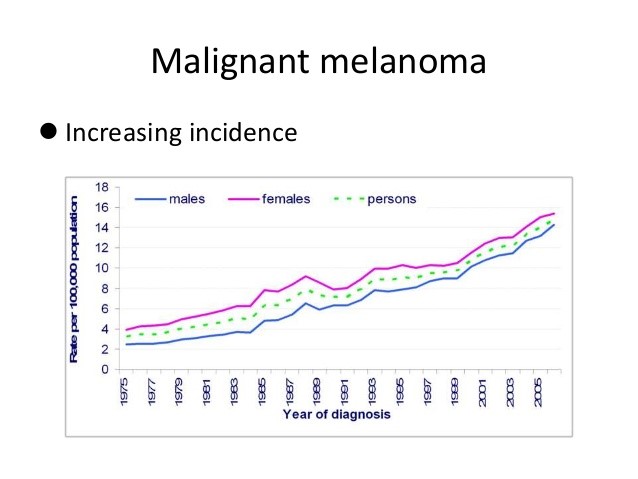
Malignant Melanoma:
Various Cancers:
Parkinson’s Incidence – Increasing in Rural areas (Farmers Using Sunscreen?)
So that’s about it, the evidence, I believe is OVERWHELMING. And that is why I call Vitamin D3 deficiency the SMOKING CANNON for the cause of many diseases as well as the cause of the many epidemics of disease the world has been experiencing since the 1980’s.
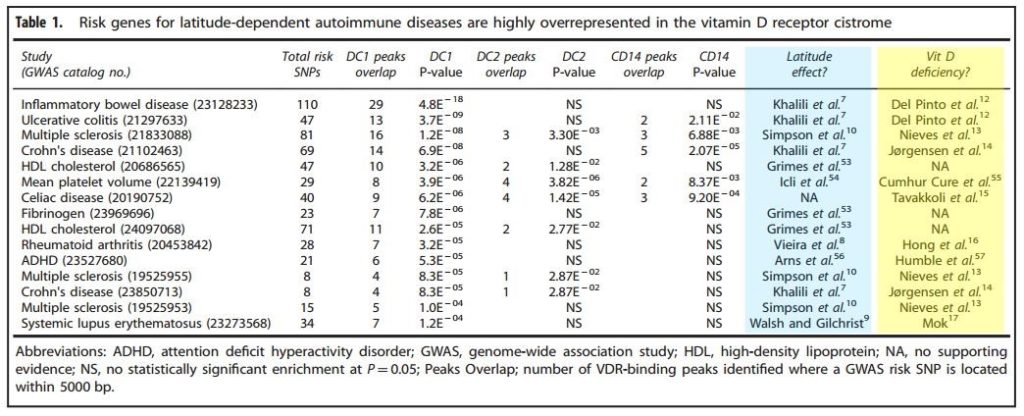
I leave you with a table that describes the genes that put you at risk for autoimmune diseases. They almost all are related to the Vitamin D3 receptor genes. The good thing is that most Vitamin D3 receptor defects can be overcome simply by taking much higher doses of Vitamin D3.
PS – PLEASE SHARE this information with all your friends and family….help spread the word…. (see share buttons below)
PPS- From time to time, as I find additional diseases or conditions that show a latitude effect and/or an increase after 1980 effect and thus will likely be treatable with long-term, high-dose Vitamin D3 for 6 to 12 months (the time it takes to remodel one’s immune system back to normal) I will add them here at the end of the article (please don’t forget to click the share button at the end!) Don’t be a freeloader!- It is bad luck!! Just click the share buttons for a GOOD KARMA boost!
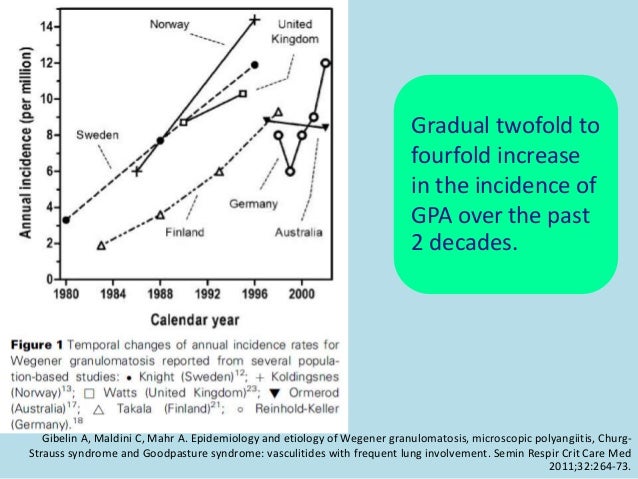
-Wegner’s Disease and Vasculitis
Wegener’s granulomatosis: epidemiological and clinical features in a …
Author information: (1)Department of Human Immunology, Institute of Medical and Veterinary Science, Adelaide, South Australia, Australia. pravin.hissaria@imvs.sa.gov.au. BACKGROUND: The epidemiology of Wegener’s granulomatosis (WG) has shown a latitude-dependent predisposition in Northern Hemisphere and in …
Wegener’s granulomatosis in New Zealand: evidence for a latitude …
Abstract. BACKGROUND: The aim of the study was to determine whether there was evidence for a geographic gradient in the incidence of Wegener’s granulomatosis (WG) and WG-like disease in New Zealand (NZ). METHODS: The National Minimum Dataset of the Ministry of Health, NZ was searched for individual patient …
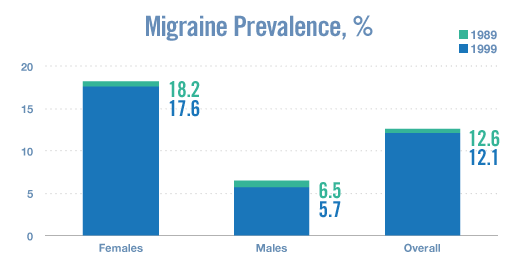
‘Migraines- There appears to be a latitiude gradient suggesting it is Vitamin D3 related

Treatment for Headache Prevalence Vs. Latitude
And another great clue! Almost every Vitamin D3 deficiency related disease is seen in women at a much higher rate than men FYI (except autism-unless oyu consider that a disease of the birth mother)…
-Vitiligo


Gender Differences in Clinicoepidemiological Features of Vitiligo: A …
Feb 13, 2014 – We used logistic regression models to estimate the association between gender and clinical characteristics of vitiligo and to evaluate the factors …. Males were significantly less likely to report onset of vitiligo in the age of 25 to 45 years compared with females in our population (odds ratio(OR): 0.38, 95% ..
High-Dose Vitamin D Dramatically Improves Psoriasis and Vitiligo
www.greenmedinfo.com/…/high-dose-vitamin-d-dramatically-improves-psoriasis-and…
Sep 9, 2017 – A pilot study illuminates that high-dose vitamin D significantly improves lesions and depigmentation in psoriasis and vitiligo, respectively. Because Vitamin D deficiency is implicated in the pathophysiology of autoimmune responses, these findings may be applicable to other autoimmune disorders.
Ovarian Cancer-
Link Between Ovarian Cancer,
Vitamin D Status Seen Worldwide
October 31, 2006
By Nancy Stringer
Using newly available data on worldwide cancer incidence, researchers at the Moores Cancer Center at UCSD have shown a clear association between deficiency in exposure to sunlight, specifically ultraviolet B (UVB), and ovarian cancer. UVB exposure triggers photosynthesis of vitamin D3 in the body. This form of vitamin D also is available through diet and supplements.

Anaphylaxis-an acute allergic reaction to an antigen (e.g., a bee sting) to which the body has become hypersensitive.
ADHD-
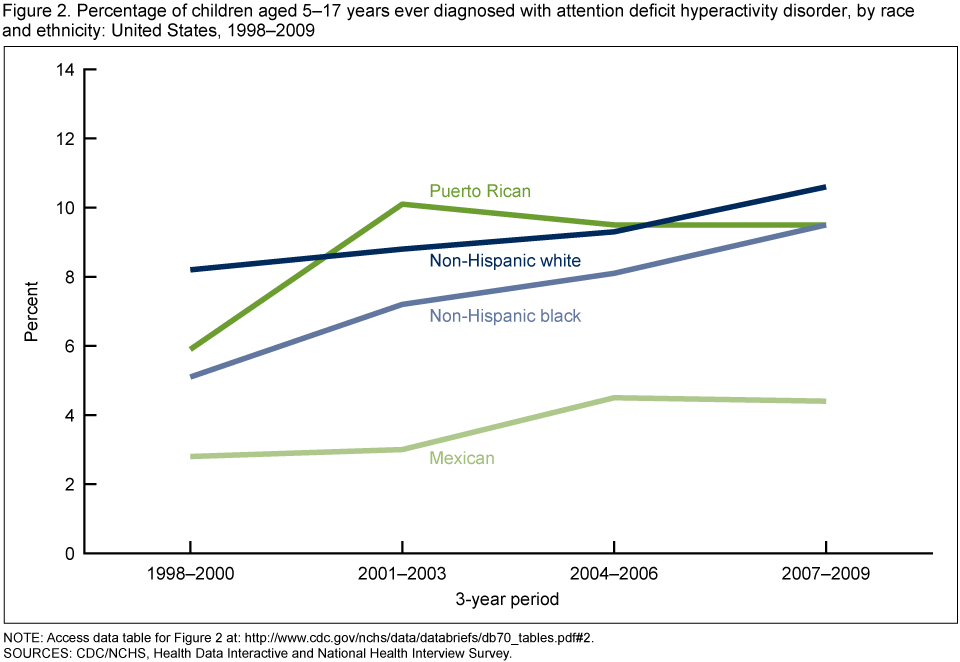
Biol Psychiatry. 2013 Oct 15;74(8):585-90. doi: 10.1016/j.biopsych.2013.02.010. Epub 2013 Mar 21.
Geographic variation in the prevalence of attention-deficit/hyperactivity disorder: the sunny perspective.
Arns M1, van der Heijden KB, Arnold LE, Kenemans JL.
BACKGROUND:Attention-deficit/hyperactivity disorder (ADHD) is the most common psychiatric disorder of childhood, with average worldwide prevalence of 5.3%, varying by region.
METHODS:We assessed the relationship between the prevalence of ADHD and solar intensity (SI) (kilowatt hours/square meters/day) on the basis of multinational and cross-state studies. Prevalence data for the U.S. were based on self-report of professional diagnoses; prevalence data for the other countries were based on diagnostic assessment. The SI data were obtained from national institutes.
RESULTS: In three datasets (across 49 U.S. states for 2003 and 2007, and across 9 non-U.S. countries) a relationship between SI and the prevalence of ADHD was found, explaining 34%-57% of the variance in ADHD prevalence, with high SI having an apparent preventative effect. Controlling for low birth weight, infant mortality, average income (socioeconomic status), latitude, and other relevant factors did not change these findings. Furthermore, these findings were specific to ADHD, not found for the prevalence of autism spectrum disorders or major depressive disorder.
CONCLUSIONS:In this study we found a lower prevalence of ADHD in areas with high SI for both U.S. and non-U.S. data. This association has not been reported before in the literature. The preventative effect of high SI might be related to an improvement of circadian clock disturbances, which have recently been associated with ADHD. These findings likely apply to a substantial subgroup of ADHD patients and have major implications in our understanding of the etiology and possibly prevention of ADHD by medical professionals, schools, parents, and manufacturers of mobile devices.
Lung Cancer-

Interestingly, once you get lung cancer, having high levels of Vitamin D3 improves your odds of surviving!!!! Can even highe levelsof D3 cure one’s cancer????We need to do the experiments…ourselves,,,,,,Big Pharma won’t !
and the chart below suggests a dosage effect. Note the highest dose of 81 nmol/L converts to 32 ng/ml which is the US measure. The US reference range is 30 to 100 ng/ml , and lifeguards routinely achieve D3 levels of 125 ng/ml. It would be interesting to see what effect a blood level of 150 ng/ml+ of D3 would have on lung cancer outcomes! Data like this suggests that high dose D3 might even be a good treatment for cancer. I will have to look into this soon.
Also, lung cancer rates for never-smokers is jumping dramatically in recent years , MORE THAN DOUBLING since 1990, and is found, like every other vitamin D3 deficiency related disease, at a much higher rate in women than in men.
“Evaluating comparable groups of males and females, rates of non–smoking-associated lung cancer were consistently higher among females in the NHS, MEC, U/OLCR, and NHEFS cohorts compared with males in the HPFS, MEC, U/OLCR, and NHEFS cohorts. The higher rate among females suggests sex-based differences in either susceptibility or exposure to risk factors (such as secondhand smoke) for non–smoking-associated lung cancer.”
From- THORACIC ONCOLOGY Journal of Clinical Oncology – published online before print September 21, 2016-Lung Cancer Incidence in Never Smokers
Medscape Medical News from the
Lung Cancer Rates Surging in Never-Smokers Roxanne Nelson September 09, 2015
The second study demonstrated that the incidence of lung cancer in never-smokers is increasing in the United States. This was observed in three facilities, most significantly for NSCLC. At one institution, for example, the rate of never-smokers climbed from 8.9% in 1990–1995 to 19.5% in 2011–2013.
Prostate Cancer-


Dementia/Azheimer’s-
From Epidemiology. Author manuscript; available in PMC 2016 Mar 1.Epidemiology. 2015 Mar; 26(2): 263–270.Geographical variation in dementia:
examining the role of environmental factors in Sweden and Scotland
Dementia rates may vary with latitude
Now it seems the risk of developing dementia might be greater for people at higher latitudes.Dementia is a catch-all term for several conditions that impair mental functioning seriously enough to interfere with daily life, such as Alzheimer’s disease.It’s well-established that genetics play a role in causing dementia. But there’s been little research on environmental factors that might be involved.Public health officials generally assume that dementia is equally common everywhere you go. So, an international group of researchers decided to see if that assumption should be challenged.Their findings were published in a recent issue of the journal Epidemiology.The study involved health data on older people, including about twenty-seven-thousand older twins living in Sweden.The results showed that if one twin lived further north than the other, the overall dementia risk was two or three times greater for that twin, compared with the one farther south.

Parkinson’s Disease-
Oddly, this disease is seen at a 50% higher rate in men than women which is rare amongst Vitamin D3 deficiency related diseases. Possibly occupational factors come into play and if these were factored out the sex ratio would reverse?
Cholesterol Levels-


Cataracts-
This is a tricky one because it is thought that exposure to UV light increases the incidence of cataracts, however, it also increases Vitamin D3 levels which should counteract cataracts via eye lens remodeling. A better study would be to compare Vitamin D3 levels to incidence of cataracts to attempt to remove the confounding variable of possible UV damage to the eye.
So here is information on that question>>
Vitamin D deficiency and posterior subcapsular cataract. – NCBI
In five early-stage PSC (cataracts) patients taking 5,000 IU of 25-OH D daily for vitamin D deficiency, there was resolution of their cataracts during the 2-year follow-up period. CONCLUSION: Vitamin D levels for most PSC patients fell below the 30 ng/mL calcium homeostasis threshold.Jun 16, 2015
Original Investigation
March 2016 Geogrpahic Variation in the Rate and Timing of Cataract Surgery Among US Communities
Courtny, Y; Taylor S. Blachley, MS1; Paul R. Lichter, MD, MS1; et al
Importance Previous studies using data from the 1980s found relatively little geographic variation in cataract surgery rates across the United States. We do not know whether similar patterns hold true today, nor do we know the patient- and community-level factors that might explain any recent geographic variations in the rate and timing of cataract surgery.

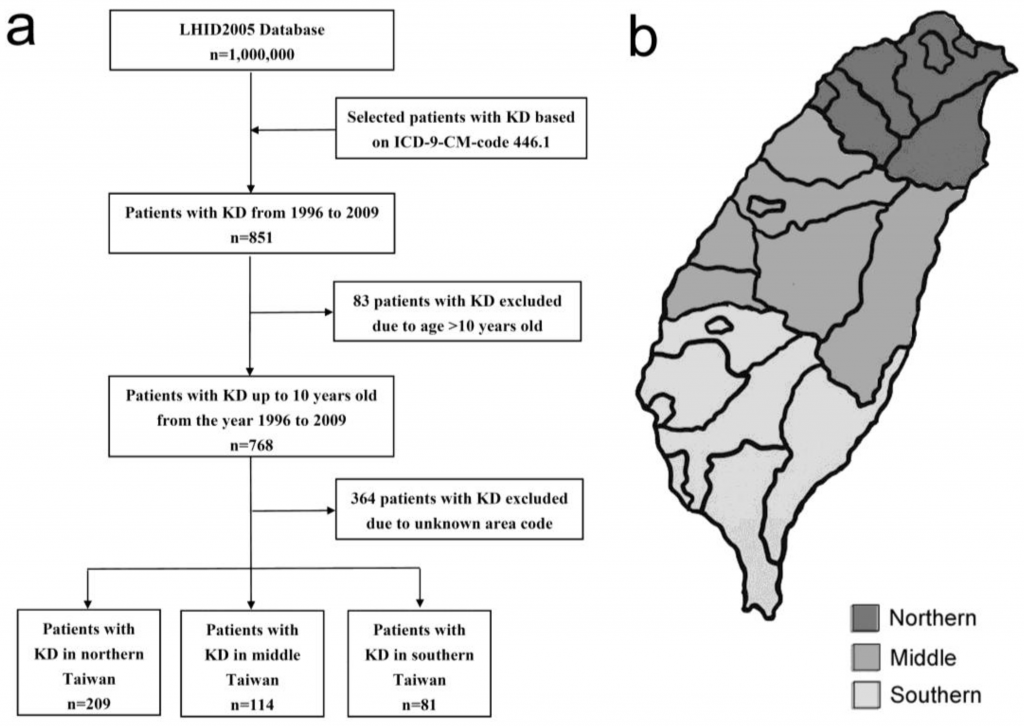
Kawasaki Disease-
Because Kawasaki Disease has shown an explosive rise in incidence in the past few decades, it is likely caused by increased sunscreen use/sun avoidance>>>Vitamin D3 deficiency >>>>>and thus can be cured by long term high dose Vitamin D3 therapy>>>>
Upon furher investigation, I have discovered thatthis disease attacks out of the blue and can be fatal within 10 days…..So the likely best treatment for this would be high dose Vitamin D3 , maybe 50,000iu per day for 5 days….but also do what your doctor says as well!!

| Region | Latitude | Incidence a | Period | Citation |
|---|---|---|---|---|
| Asia | ||||
| Japan | 24–46 | 264.8 | 2012 | Makino et al. 2015 [7] |
| Korea | 33–39 | 194.7 | 2014 | Kim et al. 2017 [9] |
| Beijing | 39 | 55.1 | 2004 | Du et al. 2007 [12] |
| Shanghai | 31 | 55.5 | 2012 | Chen et al. 2016 [13] |
| Taiwan | 22–25 | 69.0 | 2003–2006 | Huang et al. 2009 [14] |
| Hong Kong | 22 | 39.0 | 1994–2000 | Ng et al. 2005 [15] |
| India | 8–37 | 7.0 | 2014 | Singh et al. 2016 [10] |
| Thailand | 5–20 | 2.6 | 2002 | Durongpisitkul et al. 2006 [11]
|
| North America | ||||
| Canada | 41–83 | 26.2 | 1995–2006 | Lin et al. 2010 [16] |
| United States | 18–71 | 20.8 | 2006 | Holman et al. 2010 [17]
|
| Europe | ||||
| Finland | 59–70 | 11.4 | 1998–2009 | Salo et al. 2012 [18] |
| Norway | 57–80 | 5.4 | 1998–2009 | Salo et al. 2012 [18] |
| Sweden | 55–69 | 7.4 | 1998–2009 | Salo et al. 2012 [18] |
| Ireland | 51–55 | 15.2 | 1996–2000 | Lynch et al. 2003 [19] |
| Netherlands | 50–53 | 5.8 | 2008–2012 | Tacke et al. 2014 [20] |
| England | 49–60 | 8.4 | 1998–2003 | Harnden et al. 2009 [21] |
| Germany | 47–54 | 7.2 | – | Jakob et al. 2016 [22] |
| France | 42–51 | 9.0 | 2005–2006 | Heuclin et al. 2009 [23] |
| Portugal | 37–42 | 6.5 | 2000–2011 | Pinto et al. 2017 [24] |
| Italy | 35–47 | 14.7 | 2008–2013 | Cimaz et al. 2017 [25] |
Severe vitamin D deficiency in patients with Kawasaki disease: a potential role in the risk to develop heart vascular abnormalities?
Abstract
Twenty-five-hydroxyvitamin D (25(OH)-vitamin D) is crucial in the regulation of immunologic processes, but-although its deficiency has been reported in patients with different rheumatological disorders-no data are available for Kawasaki disease (KD). The goals of this study were to assess the serum levels of 25(OH)-vitamin D in children with KD and evaluate the relationship with the eventual occurrence of KD-related vascular abnormalities. We evaluated serum 25(OH)-vitamin D levels in 79 children with KD (21 females, 58 males, median age 4.9 years, range 1.4-7.5 years) in comparison with healthy sex-/age-matched controls. A significantly higher percentage of KD patients (98.7 %) were shown to have reduced 25(OH)-vitamin D levels (<30 ng/mL) in comparison with controls (78.6 %, p < 0.0001). Furthermore, KD patients had severely low levels of 25(OH)-vitamin D than controls (9.17 ± 4.94 vs 23.3 ± 10.6 ng/mL, p < 0.0001), especially the subgroup who developed coronary artery abnormalities (4.92 ± 1.36 vs 9.41 ± 4.95 ng/mL, p < 0.0001). In addition, serum 25(OH)-vitamin D levels correlated not only with erythrosedimentation rate (p < 0.0001), C-reactive protein (p < 0.0001), hemoglobin level at KD diagnosis (p < 0.0001) but also with both coronary artery aneurysms (p = 0.005) and non-aneurysmatic cardiovascular lesions (p < 0.05). Low serum concentrations of 25(OH)-vitamin D might have a contributive role in the development of coronary artery complications observed in children with KD.
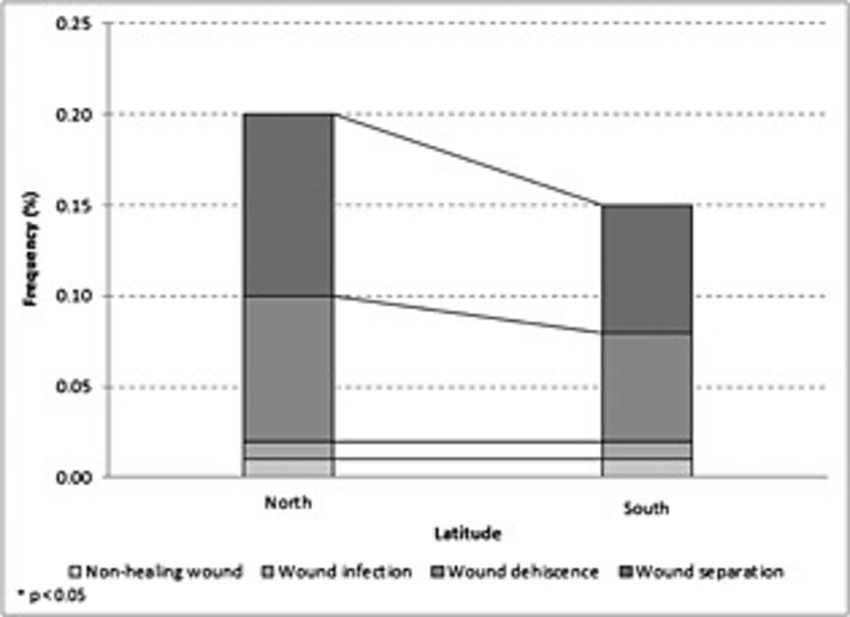
Chronic Wounds-
Just did a search of chronic wounds vs latitude to see if there is some sort of latitude gradient for chronic wound incidence which would suggest a Vitamin D3 connection. (Because the sun is stronger at the equator and thus Vitamin D3 (which is made in your skin when the sun hits it) levels are presuemd to be higher in humans on average, and decline as one moves further from the equator.) I did find this article>>>
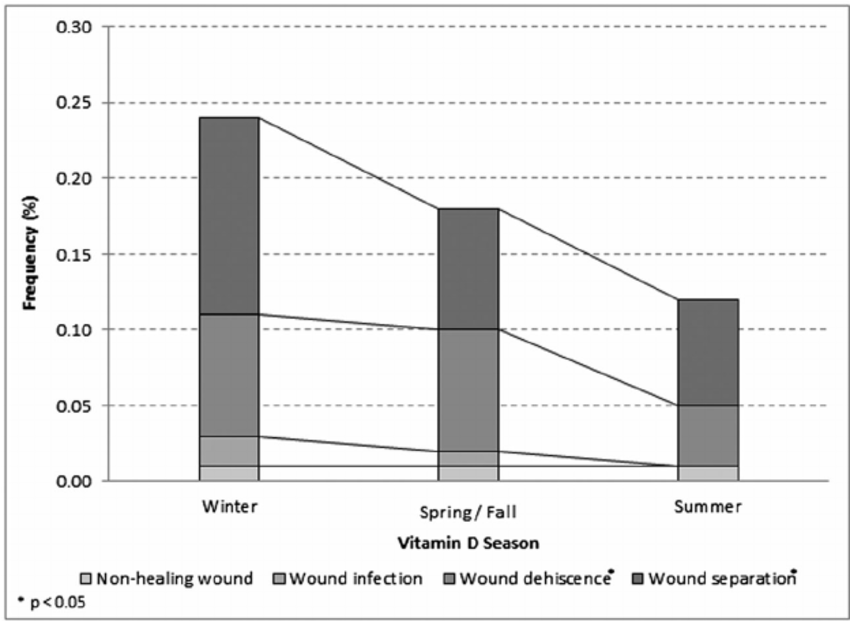
You might want to read about a woman who cured her chronic wound of 3 years by taking 80,000 iu’s per day of Vitamin D3..in just 3 weeks!>>>>
Vitamin D3 Case Study #4: 3-Year Dangerous Chronic Wound Completely Healed in 3 Weeks
SIDS (SUDDEN INFANT DEATH SYNDROME)
Yes there is evidence that SIDS is caused by Vitamn D3 deficiency as well.
New Research Links Vitamin D Deficiency and SIDS in Infants
by Katlyn Joy | March 9, 2012 9:53 AM0 Comments
In January 2012, researchers from the Royal London Hospital and Sheffield Children’s Hospital, noted that one in four youngsters have Vitamin D deficiency and believe there could be a link between this nutritional lack and the incidence of Sudden Infant Death Syndrome or SIDS.
Vitamin D deficiency can cause rickets, a disorder that results in weakened and brittle bones. Rickets is caused by too little Vitamin D, calcium or phosphate. Children with this disorder may easily receive bone fractures. This may result in suspicion of child abuse, when children have multiple fractures or a repeated history of bone breaks.
Vitamin D deficiency is more commonly seen in African American children because their increased pigmentation means less absorption of sunlight and the associated Vitamin D. Rates of both SIDS and Vitamin D deficiency are higher in African American children. Both conditions are also known to peak during low sunlight winter months as well.
Another consideration is breastfeeding. Breastfed infants require Vitamin D supplements beginning by two months of age. The recommended amount of Vitamin D supplement is 400 IUs daily. These are usually administered as drops to the infant.
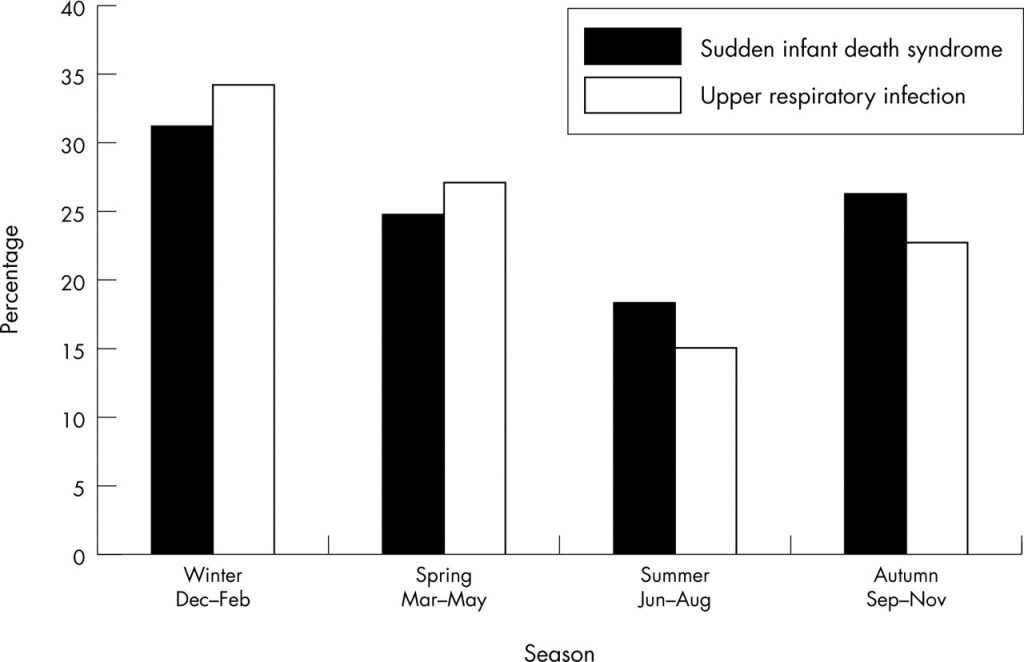
Contradictory evidence to the idea that SIDS is caused by Vitamin D3 deficiency is found in the fact that SIDS deaths have been declining quite a bit since the 1980’s. However this might be due to widespread parental training in how to prevent SIDS by making sure the baby sleeps on his or her back, and the removal of all toys and objects from the crib at night.
AMD (Advanced Macular Degeneration)-
This is a complicated disease to untangle, much like catartacts, because sun exposure both increases the incidence of AMD, but it also leads to higher levels of Vitamin D3 which is AMAZINGLY protective against AMD- reducing its incience by 83%! See article below… So it will also be hard to see an increase in incidence over time because sun avoidance adds a confounding variable..Nonetheless, it is my expectation that high dose vitamin D3 has a very good chacne to reverse AMD-I have seen anecdotal reports here and there on the web that this is true.
Low Vitamin D Levels Linked to Macular Degeneration Risk
“The findings of the present meta-analysis strengthen the idea that there might be a link between vitamin D deficiency and AMD, notably at the late stages of the disease (P=0.002),” write Cedric Annweiler, MD, PhD, from Angers University Hospital in France, and colleagues. “It may therefore be possible that correction of vitamin D deficiency could improve the prognosis of AMD.”
The researchers used a Medline search through November 2015 to identify 11 studies that met their selection criteria, out of an initial 243 found. The criteria included observational or interventional studies and outcomes based on data about AMD diagnoses (in at least one eye) and circulating vitamin D concentration.
Among the studies, seven were cross-sectional, one was a case series, one was a case–control study, one was a retrospective longitudinal cohort study, and one was a discordant sibling cohort. They ranged in size from 65 to 17,045 participants; from 31 to 1440 participants had AMD. The researchers categorized AMD as whole, early, or late. All the studies had been published since 2007.
In a second analysis, those in the highest quintile of circulating vitamin D levels had the lowest odds of AMD compared with those in the lowest quintile. Those with the highest vitamin D levels had 83% lower odds of AMD (odds ratio [OR], 0.83; 95% CI, 0.71 – 0.97) and 47% lower odds of late AMD (OR, 0.47; 95% CI, 0.28 – 0.79) compared with those with the lowest levels.
Another odd fact I discoverd is that people who take aspirin on a regular basis have a huge increase in the risk of AMD. Does aspirin cause AMD or is it just more prevalent in those with heart disease who take aspriin..that I do not know at this time>>
ALS (Amyotrophic Lateral Sclerosis)- Fits the pattern exactly. Note ALS has been successfully reversed in a mouse model of ALS by progesterone, which suggests more research is needed to see if progesterone and Vitamin D3 have overlapping duties in the endocrine system. This seems a good area to research in that both hormones, Vitamin D3 and Progesterone modulate the immune system. In the case of Progesterone high levels help tame the mother’s immune system to prevent attack of the fetus, whil Vitamin D3 can turn of the immune system attack in all autoimmune diseases.
-Vitamin D as a potential therapy in amyotrophic lateral sclerosis (mouse ALS) – Feb 2014
CNS Neurosci Ther. 2014 Feb;20(2):101-11. doi: 10.1111/cns.12204.
–Neurobiol Dis. 2013 Nov;59:80-5. doi: 10.1016/j.nbd.2013.07.011. Epub 2013 Jul 26.
Autophagy activation and neuroprotection by progesterone in the G93A-SOD1 transgenic mouse model of amyotrophic lateral sclerosis
Figure 3. Cumulative incidence of neovascular age-related macular degeneration by time intervals. Cumulative incidence was estimated using the Kaplan-Meier (product limit) method.
![THE ALS PUZZLE SOLVED? A THEORY OF WHY TWO HARMLESS OFF THE SHELF HORMONES SHOULD STOP ALS IN ITS TRACKS! by [BOWLES, JEFF T.]](https://images-na.ssl-images-amazon.com/images/I/515pUAc76mL.jpg)
The Big Vitamin D Mistake
Abstract
Since 2006, type 1 diabetes in Finland has plateaued and then decreased after the authorities’ decision to fortify dietary milk products with cholecalciferol. The role of vitamin D in innate and adaptive immunity is critical. A statistical error in the estimation of the recommended dietary allowance (RDA) for vitamin D was recently discovered; in a correct analysis of the data used by the Institute of Medicine, it was found that 8895 IU/d was needed for 97.5% of individuals to achieve values ≥50 nmol/L. Another study confirmed that 6201 IU/d was needed to achieve 75 nmol/L and 9122 IU/d was needed to reach 100 nmol/L. The largest meta-analysis ever conducted of studies published between 1966 and 2013 showed that 25-hydroxyvitamin D levels <75 nmol/L may be too low for safety and associated with higher all-cause mortality, demolishing the previously presumed U-shape curve of mortality associated with vitamin D levels. Since all-disease mortality is reduced to 1.0 with serum vitamin D levels ≥100 nmol/L, we call public health authorities to consider designating as the RDA at least three-fourths of the levels proposed by the Endocrine Society Expert Committee as safe upper tolerable daily intake doses. This could lead to a recommendation of 1000 IU for children <1 year on enriched formula and 1500 IU for breastfed children older than 6 months, 3000 IU for children >1 year of age, and around 8000 IU for young adults and thereafter. Actions are urgently needed to protect the global population from vitamin D deficiency.
INTRODUCTION
The incidence of type 1 diabetes (T1D) has been doubling every 20 years. In Finland, the recommendation for daily vitamin D supplementation was gradually reduced from 4000-5000 IU in 1964 to 400 IU in 1992. Concomitantly, T1D increased by 350% in those aged 1-4 years, 100% in those aged 5-9 years, and 50% in those aged 10-14 years [1]. However, since 2006, T1D has plateaued and decreased after an increase in serum 25-hydroxyvitamin D (25[OH]D) after the authorities’ decision to fortify all dietary milk products with cholecalciferol [2]. Moreover, the worldwide association of ultraviolet (UV)-B light and vitamin D status with T1D and multiple sclerosis is now more than evident.
MAIN BODY
Vitamin D and Immunomodulation
The role of vitamin D in innate and adaptive immunity is critical. It has been shown that the redirection of human autoreactive T-cells upon interaction with dendritic cells can be modulated by an analog of 1,25-dihydroxyvitamin D3 [3]. In a recent plenary session entitled “Cell Therapy in Type 1 Diabetes” that closed the 2016 meeting of the European Society for Paediatric Endocrinology in Paris, Bart O. Roep [3] announced the initiation of phase 1 clinical trials in humans in 2016 with the following protocol: dendritic cells will be isolated from the patient’s peripheral blood, cultured with calcitriol, and then re-injected in an abdominal intradermal position to ‘teach’ the rest of the immune cells not to attack β-cells anymore. In a large birth cohort study, T1D incidence was reduced by 78% with 2000 IU of cholecalciferol per day [4]. Moreover, T1D autoantibodies can be “negativated” with oral calcitriol [5]. Vitamin D levels >100 nmol/L (40 ng/mL with a conversion factor of ×2.5) improve insulin secretion [6] and prevent β-cell destruction by suppressing macrophage adhesion and migration through downregulation of endoplasmic reticulum stress and scavenger receptor-A1 [7].
The Statistical Error in the Estimation of the Recommended Dietary Allowance of Vitamin D
Veugelers and Ekwaru [8], in a correct reanalysis of the data used by the Institute of Medicine, proved that 8895 IU/d are needed for 97.5% of individuals to achieve values ≥50 nmol/L. Heaney et al. [9] confirmed that finding, reporting that 6201 IU/d were needed to achieve the Endocrine Society’s recommendation of 75 nmol/L and 9122 IU/day to reach 100 nmol/L.
What Serum Vitamin D Levels Should We Aim for?
Garland et al. [10] published the largest meta-analysis ever conducted of all studies published between January 1, 1966 and January 15, 2013 dealing with all-cause mortality related to serum 25(OH)D, showing that 25(OH)D levels <75 nmol/L may be too low for safety and associated with higher all-cause mortality, demolishing the U-shape curve of vitamin D levels and mortality that had been assumed until then.
Call to Public Health Authorities
Since all-disease (autoimmune diseases, metabolic syndrome, type 2 diabetes, cancer) mortality risk is reduced to 1.0 with serum vitamin D levels ≥100 nmol/L [10], we call all responsible public health authorities to consider designating as the recommended dietary allowance (i.e., the average daily level of intake sufficient to meet the nutrient requirements of nearly all healthy people, presuming minimal sun exposure) intake levels corresponding to those proposed by the Endocrine Society Expert Committee (2011) as safe upper tolerable daily intake doses for patients at risk for vitamin D deficiency (<50 nmol/L): 2000 IU for those <1 year of age, 4000 IU for those aged 1-18 years, and 10 000 IU for those aged >18 years.
Since 10 000 IU/d is needed to achieve 100 nmol/L [9], except for individuals with vitamin D hypersensitivity, and since there is no evidence of adverse effects associated with serum 25(OH)D levels <140 nmol/L, leaving a considerable margin of safety for efforts to raise the population-wide concentration to around 100 nmol/L, the doses we propose could be used to reach the level of 75 nmol/L or preferably 100 nmol/L. Of course, these recommended doses can be individualized based on dietary and sun exposure habits and the latitude of the country, and they can also be adjusted according to body mass index, age, and skin color, with obese, elderly, and dark-skinned people needing higher doses.
Explanation of the Pandemic of Vitamin D Deficiency
Only 20% of our vitamin D reserve is meant to come from the diet. The remaining 80% is expected to be produced in our skin from the UV-B of the sun. In contrast to the context of the recommendations of the 1960s of 4000 to 5000 IU/d to avoid rickets, our diet today is poor in wild fish (×10 richer in vitamin D), wild eggs, and fresh milk. Children are playing and people are working indoors all day long, and powerful sunprotective cosmetics are used to prevent melanoma. Even sunny countries such as Greece present a high prevalence of vitamin D deficiency, as the angle of the sun rays from autumn to spring do not result in sufficient vitamin D production with usual sun exposure.
Optimal Vitamin D Supplementation
With the target for vitamin D set at 100 nmol/L, the dose, frequency, and duration of supplementation will be important factors for healthy subjects committed to optimizing their nutritional status. Since in the case of vitamin D, serum levels depend on dietary intake (20%) and sun exposure (80%), a practical approach would be to recommend at least the three-fourths of the upper tolerable dose proposed by the Endocrine Society to be taken as a supplement all year long except for circumstances such as vacations in which one engages in sunbathing. This could translate to, for instance, 1000 IU for children <1 year on enriched formula and 1500 IU for those older than 6 months who are breastfed, 3000 IU for children >1 year of age, and up to 8000 IU for young adults and thereafter, with non-pediatric doses adapted to the body mass index with the target set to 100 nmol/L instead of 50 nmol/L. More importantly, according to the Endocrine Society’s clinical practice guidelines, doses up to 1000 IU/d for infants up to 6 months, 1500 IU/d for infants from 6 months to 1 year, 2500 IU/d for children aged 1-3 years, 3000 IU/d for children aged 4-8 years, and 4000 IU/d for everyone over 8 years can be given safely without medical supervision just to prevent vitamin D deficiency, while higher doses may be needed to correct hypovitaminosis D.
Importance of Vitamin D Supplementation
Such a strategy relies on adequate supplementation among pregnant and lactating women, and on timely supplementation of every newborn before seroconversion towards autoimmune targets occurs. The benefits for individuals’ general health status, apart from the obvious gains in skeletal health, cannot be fully foreseen, but may very well be surprisingly greater than expected given the impact of vitamin D deficiency on metabolic syndrome itself. Improvements in vitamin D status may help reduce the public health burden of metabolic syndrome and of potential subsequent health conditions, including type 2 diabetes and cardiovascular disease.
CONCLUSION
Unfortunately, medicine took a very long time to realize that vitamin D is not simply a vitamin that prevents rickets. For that purpose, 400-600 IU/d may be enough. However, we know today that vitamin D is a powerful nuclear receptor-activating hormone of critical importance, especially to the immune system. With the available data mentioned above, the proposed doses would probably suffice to maintain vitamin D levels around or over 75-100 nmol/L, with practically zero risk of toxicity. Undeniably, further studies are needed to clarify the optimal supplementation of vitamin D, although it is uncertain whether a universal recommended dietary allowance is feasible. Meanwhile, actions are urgently needed to protect the global population from the threats posed by vitamin D deficiency.
(And Finally- Stop getting ripped off!)>>>>>>
Amazing research and amazing conclusion. You deserve a Noble prize.
How much Vit D3 as a supplement is suggested ?
Just searched “cleft latitude incidence” found that there seems to be a latitude effect in Europe
twice as many cleft lips and palates in Netherlands & Finland than in Italy or Portugal>>>>> https://www.omicsonline.org/open-access/cleft-lip-and-palate-etiology-epidemiology-preventive-and-intervention-strategies-2161-0940.1000150.php?aid=28428
Here’s a new article where they find autism rates vary with latitude!!
Medical Hypotheses
Volume 109, November 2017, Pages 19-24
Medical Hypotheses
A review of prevalence studies of Autism Spectrum Disorder by latitude and solar irradiance impact
Author links open overlay panelSomayyaSyedaKathleen A.MooreabEvitaMarcha
Show more
https://doi.org/10.1016/j.mehy.2017.09.012Get rights and content
Abstract
Autism Spectrum Disorder (ASD) is a lifelong disability with no known cause or cure. Among the suggested etiologies, is Cannell’s hypothesis of a deficiency in Vitamin D the main natural source of which is Solar Ultraviolet-B (UVB) radiation. The aim in this paper is to build on this hypothesis and explore the relationship of solar irradiance of which UVB is a component, by latitude with the prevalence rates of ASD. Twenty-five reports published between 2011 and 2016 using comparable diagnostic criteria were reviewed. The results suggest a tendency for the prevalence rates of ASD to be lowest in countries near the equator and for this rate to increase as the latitude increases. These findings provide some support not just for the Vitamin D hypothesis, but also for a new proposition that along with UVB radiation, the entire solar radiation spectrum which reaches the earth, may play a role in ASD. While these results are both novel and encouraging in terms of the potential efficacy of exposure to natural sunlight, further research is warranted before results can be considered definitive, and before the implications of the findings can be implemented clinically.
Additional Proof that Vitamin D3 Deficiency is at the root cause of Wegener’s suggesting that high dose D3 can cure Wegener’s>>>
A latitude effect!>>>
Intern Med J. 2007 Apr;37(4):242-6.
Wegener’s granulomatosis in New Zealand: evidence for a latitude-dependent incidence gradient.
O’Donnell JL1, Stevanovic VR, Frampton C, Stamp LK, Chapman PT.
Author information
Abstract
BACKGROUND:
The aim of the study was to determine whether there was evidence for a geographic gradient in the incidence of Wegener’s granulomatosis (WG) and WG-like disease in New Zealand (NZ).
METHODS:
The National Minimum Dataset of the Ministry of Health, NZ was searched for individual patient discharges coded by the International Classification of Diseases 10th Revision, Australian Modification as either M301 (polyarteritis with lung involvement, including Churg Strauss and allergic granulomatous angiitis) or M313 (WG, necrotizing respiratory granulomatosis) for the period 1 January 1999 to 31 December 2003. Data were standardized using the 2001 NZ census.
RESULTS:
One hundred and ninety-five patients (95 men) were given a first-time discharge code of either M301 (40 patients) or M313 (155 patients). No gender bias was seen. The rate among Europeans was twice that of NZ Maoris or Asians. The rate of disease peaked in the age band 70-79 years and during winter months. A significant positive north-south geographic gradient was present for M313. No difference in the rate of readmission or time to relapse between geographic regions was found for M313.
CONCLUSION:
A north-south gradient in the rate of patient discharges given a diagnostic code of M313 (WG, necrotizing respiratory granulomatosis) was present in NZ. This finding supports the hypothesis that there is a latitude-dependent risk factor(s) for WG possibly common to both global hemispheres.
PMID: 17388864 DOI: 10.1111/j.1445-5994.2006.01297.x
Found another one>>>
Cholesterol levels vary with latitude
You can ADD cataracts to the list!>>
“In five early-stage PSC (cataracts) patients taking 5,000 IU of 25-OH D daily for vitamin D deficiency, there was resolution of their cataracts during the 2-year follow-up period. CONCLUSION: Vitamin D levels for most PSC patients fell below the 30 ng/mL calcium homeostasis threshold.Jun 16, 2015”
Vitamin D deficiency and posterior subcapsular cataract
Craig J Brown,1 Faical Akaichi2
1The Eye Center, Fayetteville, AR, USA; 2Scotland’s Rural College, Edinburgh, UK
Purpose: To evaluate risk factors associated with posterior subcapsular cataract (PSC) development and the relationship between vitamin D deficiency and etiology of PSC.
Methods: Of 195 consecutive patients from a private ophthalmology practice, diagnosed with PSC, serum vitamin D3 (25-OH D) levels were obtained for 175, and associations among risk factors, comorbidities, and PSC were assessed.
Results: In all 175 PSC patients, mean 25-OH D levels were low (24 ng/mL ±11 SD) compared with age/sex-matched standards. Significant differences in 25-OH D levels were noted between PSC subjects taking/not taking calcium supplements, systemic steroids, osteoporosis medications, etc. Alone, smoking status and calcium channel blockers and/or topical steroids use made no significant difference in PSC subjects 25-OH D levels, but two or more of these factors were associated with lowered levels of 25-OH D (P<0.001). Low vitamin D was correlated with female sex, autoimmune disease, and non-skin cancer diagnosis, but not with age, or other comorbidities or medication use. In five early-stage PSC patients taking 5,000 IU of 25-OH D daily for vitamin D deficiency, there was resolution of their cataracts during the 2-year follow-up period.
Conclusion: Vitamin D levels for most PSC patients fell below the 30 ng/mL calcium homeostasis threshold. Some comorbidities and non-ophthalmic interventions are associated with the development of PSC at less depressed levels of 25-OH D. In this series, vitamin D deficiency was associated with PSC cataract, suggesting that raising the level of vitamin D intake may reduce PSC incidence.
Here’s another one>>>Kawasaki Disease>>>
Kawasaki Disease-
Because Kawaki Disease has shown an explosive rise in incidence in the past few decades, it is likely caused by increased sunscreen use/sun avoidance>>>Vitamin D3 deficiency and thus can be cured by long term high dose Vitamin D3 therapy>>>>
Clin Rheumatol. 2016 Jul;35(7):1865-72. doi: 10.1007/s10067-015-2970-6. Epub 2015 May 22.
Severe vitamin D deficiency in patients with Kawasaki disease: a potential role in the risk to develop heart vascular abnormalities?
Stagi S1, Rigante D2, Lepri G3, Matucci Cerinic M3, Falcini F4.
Author information
Abstract
Twenty-five-hydroxyvitamin D (25(OH)-vitamin D) is crucial in the regulation of immunologic processes, but-although its deficiency has been reported in patients with different rheumatological disorders-no data are available for Kawasaki disease (KD). The goals of this study were to assess the serum levels of 25(OH)-vitamin D in children with KD and evaluate the relationship with the eventual occurrence of KD-related vascular abnormalities. We evaluated serum 25(OH)-vitamin D levels in 79 children with KD (21 females, 58 males, median age 4.9 years, range 1.4-7.5 years) in comparison with healthy sex-/age-matched controls. A significantly higher percentage of KD patients (98.7 %) were shown to have reduced 25(OH)-vitamin D levels (<30 ng/mL) in comparison with controls (78.6 %, p < 0.0001). Furthermore, KD patients had severely low levels of 25(OH)-vitamin D than controls (9.17 ± 4.94 vs 23.3 ± 10.6 ng/mL, p < 0.0001), especially the subgroup who developed coronary artery abnormalities (4.92 ± 1.36 vs 9.41 ± 4.95 ng/mL, p < 0.0001). In addition, serum 25(OH)-vitamin D levels correlated not only with erythrosedimentation rate (p < 0.0001), C-reactive protein (p < 0.0001), hemoglobin level at KD diagnosis (p < 0.0001) but also with both coronary artery aneurysms (p = 0.005) and non-aneurysmatic cardiovascular lesions (p < 0.05). Low serum concentrations of 25(OH)-vitamin D might have a contributive role in the development of coronary artery complications observed in children with KD.
Vitamin D tocicity is quite rare adn easy to correct, a new article>>
Vitamin D toxicity is rare, and usually a result of accidental overdosing, according to recent study
Posted on: January 24, 2018 by Vitamin D Council
Interest in vitamin D supplementation and testing has increased over the last few decades. Therefore, it’s only rational for concerns over toxicity and side effects to increase as well. A 16-year retrospective study evaluated the vitamin D status of patients at the University of Iowa Hospitals and Clinics (UIHC) to determine the risk of toxicity.
Researchers studied a total of 73,779 hospital patients and analyzed 127,932 serum blood samples to determine 25(OH)D status. For individuals with vitamin D levels above 120 ng/ml (300 nmol/l), or who displayed signs and symptoms of hypercalcemia, detailed medical reviews were conducted. Signs and symptoms of hypercalcemia were defined as excessive thirst, excessive urination, decreased appetite, vomiting, constipation, abdominal pain, renal failure, and/or failure to thrive.
This is what the researchers found:
Only 1.05% of the participants had vitamin D levels above 80 ng/ml (200 nmol/l).
Only 0.12% had levels that exceeded 120 ng/ml (300 nmol/l).
Four patients showed symptoms of vitamin D toxicity, and three of these cases were caused by mistaken overdosing of liquid vitamin D supplements.
The last case of toxicity was allegedly due to daily supplementation of 1,000 IU, but the researchers flagged this case for potentially inaccurate history.
The researchers concluded,
“Symptomatic vitamin D toxicity is uncommon, and elevated levels of 25(OH)D do not strongly correlate with clinical symptoms or total serum/plasma calcium levels. Our study highlights the potential risks of the liquid formulation of vitamin D.”
Here’s another one! ALS>>>
ALS deaths increasing 60 % per decade – somewhat slower than other vitamin D related diseases
ALS varies with latitude – similar to most vitamin D related diseases
Amyotrophic Lateral Sclerosis: A Synthesis of Research and Clinical Practice
Vitamin D is of course important but it is unlikely by itself to be responsible for autism.
Vitamin D synthesis depends on skin color. So autism must depend on skin color if Vitamin D is the cause. I don’t think there is evidence of that.
Near the equator, you of course are more likely to have Vitamin D, but you also have more helminth infections, lower C-section rates and lower antibiotic use which all contribute to less atopy. Also, as you move away from the equator, the number of vaccines on the schedule goes up.
Autism Spectrum Disorders: A special case of vaccine-induced cow’s milk allergy?
https://www.zenodo.org/record/1034557
Epidemiological studies that ignore mechanism of disease causation are flawed and mechanistic evidence demonstrates that vaccines cause autism
https://www.zenodo.org/record/1117106
Safety studies of aluminum in vaccines lack immunotoxicity analysis of this immunological adjuvant: Ignorance or deception?
https://www.zenodo.org/record/1117242
Hello there- I think there might be some truth to parts of the vaccine causes autism theory.
I read somewhere that some vaccines had something to interfere with the immune system by suppressing vitamin d3 so that the
immune response would last longer and develop more virus antibodies I discuss that in the 2n article link below
the first article I wrote about autism has this link>>> https://jefftbowles.com/autism-vitamin-d3-deficiency-linked/
you will likely also be intersted n this article as well>>> https://jefftbowles.com/autism-cure-d3/ I think the vaccine theory is mentioned in this one.
So is there a difference in vitamin D and vitamin D3 and Vitamin D2 . And how mich vitamin D is to much to take on a daily basis?
Thank you.
Hello thjere Linda,
THanks for asking…
Vitamin D2 is the plant version of Vitamin D3 ..it is slightly different and not as effective as animal-originated Vitamin d3.
They used to make Vitamin D2 by shining UV light on mushrooms…thus it was named ergocalciferol (ergot means fungus)..
they say that Vitamin D2 is 1/4th to 1/16th as strong or effective as vitamin d3 and might cause side effects
at high doses. I wujold recommend that humans never take D2 if D3 is available.
As far as a daily dose …for curing autoimmune diseases people regularly take 1,000 IU per day per kg of body weight.
…and the smart ones take a lot of vitamin k2 with it…to prevent the only danger of high dose v itamin d3 which is excess calcium in the blood..
The highest daily dose I know of is 1,000,000 iu’s per day with lots of k2 taken by an ex heavyweight boxer
who fought the world champion..and later was stricken by the worst kind of MS- primary progressive. He is now learnign tgo walk again
and the lesions have healed..He only does this while testing his blood calcium levels regularly…as long as they are in the normal range,
any dose of vitamin d3 is safe. For people just looking for good health 10,000 to 20,000 a day is often enough.
Hi I’m on 50’000 a week how much k2 do I take with it and how much magnesium to take
Hello Yvonne…
It might be more natural to take your vitamin d3 everyday..maybe 8000 IU per day would be the same dose. As it would be more normal to get sun everyday to make your d3 in your skin….
rather than lots of sun just once a week
make sure the 50,000 kiu pill you take is NOT ergocalciferol because that is viamin d2 which is not recommended but some doctors still use it out of habit…it is made from mushrooms!
it was isolated before the animal form (D3) was isolated..
. So at that dose 8000/day I would take at least 400 mcg of vitamin k2 of the mk7 type maybe up to 800 mcg per day if you can afford it…If you take the more natural
but weaker form of k2 (mk4) then yo would want to take 2000 to 4000 mcg per day. you can get really cheap pure vitamn k2 powder from Peter at vitaspace.com
for $15 per gram…if you buy pills you can pay up to $6500 per gram!!! (Mercola) go to the taked3.com website to find peter’s information
As far as magnesium goes….just add several pills throughout the day 9not all at once) if you are taking too much you will get diarrhea
if you don’t take enough the d3 might constipate you….(but mainly at higher doses)
you might want to read the magnesium miracle by Dr Dean…thanks JB
Great job Jeff.
I have learned so much from your research over the last few weeks and I am trying to spread the word thru my family and friends.
Thank you so much for all your efforts.
I agrea with the gentleman above who said you should win the nobel prize for your work
i’m 75 and have been following your work. i have instituted a number of your suggestions by adding supplements and adjusting dosages of those things i was already taking.
please keep up the good work!
have you seen this paper published by calico (google’s human longevity arm),, and is titled:
“A window into extreme longevity; the circulating metabolomic signature of the naked mole-rat, a mammal that shows negligible senescenceyet? https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5964061/
is there some way to reach you more privately as i would like to share what i’m doing and what my results have been.
great thanks for the article … I’ll send you an email Jeff
Read your Book .. This is the most miraculous book ive read , if ever there was one..is this Big Pharmas dirty secret .. off course its possible ..Thanks a million for helping Heal using Sun Gods own powerful Sunshine Streoid !!. Your book & worrk is truly overwhelming and deserving of the highest human honors .. more power to you..
Wheres the SHARE button
Hello there ! Thanks for sharing…the share button is at the end of the article right after a section that says Conclusion it is a little facebook symbol (there is also a twitter symbol) you click on it and it gets shared thanks!! right after this>>>>
CONCLUSION
Unfortunately, medicine took a very long time to realize that vitamin D is not simply a vitamin that prevents rickets. For that purpose, 400-600 IU/d may be enough. However, we know today that vitamin D is a powerful nuclear receptor-activating hormone of critical importance, especially to the immune system. With the available data mentioned above, the proposed doses would probably suffice to maintain vitamin D levels around or over 75-100 nmol/L, with practically zero risk of toxicity. Undeniably, further studies are needed to clarify the optimal supplementation of vitamin D, although it is uncertain whether a universal recommended dietary allowance is feasible. Meanwhile, actions are urgently needed to protect the global population from the threats posed by vitamin D deficiency.
Related
LINKS TO- All Articles Available In these Blog Pages Ranked By Popularity
March 12, 2019
In “D3”
Case Studies #16-Vitamin D3 Can Prevent & CURE Erectile Dysfunction!
November 22, 2017
In “Erectile Dysfunction”
Case Studies #13 -High Dose Vitamin D3 CURES Rheumatoid Arthritis
November 17, 2017
FacebookTwitterShare
In “Rheumatoid Arthritis”
Edit
Posted in: AMD, AMD cure, Anxiety, Asthma, Asthma cure, autoimmune disease cure, Crohn’s,
I have Rheumatoid and have for years. I just found your site and D3 info. I am almost afraid to be encouraged. Question is their a certain “type” of D3 that is better? is Nordic Naturals D3 gummies 1000 IU good enough?
Hello there Debbie keep in mind that if you sit in the summer sun in a swim suit for 1/2 hour your skin will make 20,000 IU’s of D3 .
Dr Coimbra has been curing people of their RA by having them take 1,000 I’s of D3 per each KG of body weight You should google the Dr. Coimbra Protocol it is mostly for MS but
he cures RA pateints as well.
Dear Jeff,
started taking 72,000 IUs of D3 since a week, balanced with 6mg of pure K2 (mk4) for every 10K IU of D3 .
what is the advisable dosage of 10% K2 mk4 with D3 — what i have purchased from Vitaspace is K2 10% (MK-4)
My wife has had partial knee replacement and the knee is still painful and after starting the high dosage of D3 +K2 — pain has increased..
Question — does the pain increase during the healing process??
is that normal?
Thanks
Kumar
Hello Kumar
Thansk for writing…Yes pain increases for a month or two…in my case when I sarted toaking 4000 iu per day it eliomnate the cracking sounds in my shoulders and any pains….
It stayed that way for about 10 yuears..then I bumped it up to 20,000 to 25,000 a day and within a month my shoulders felt liek soemone hit them with a seldgehammer
Had a similar issue with my hip click it started really hurting so bad I had to stop taking d3 for a week or so take a lot of ibuprofen but I
powered through as I knew it was the bone and joint remodeling hormone. after abouit 2 months …viola the pain stopped and my huip click of 28 years disappeared! Apparently it was a bone spur that dissolved…So pain can be expected especially in old injuries…now I am not sure what happens with an articial knee..please report back it is of great interst
Will the body remodel some tissues around it adn accept it? or will the pain not stop after 2 months…This is an important question to answer..
As far as how much K2 tot take I reccomend a minimum of 400 micrograms = .4 mg of the mk7 type o k2 with each 10,000 iu of d3 OR 2000 mcg = 2mg of the mk4 type of k2
double this amount if you ca afford it…..And if you want to clean out your arteries of calcification I myself have taken 45 mg = 45,000 mcg 3X per day for 3 months…K2 is not toxic apparently in any dose….You should also be taking mgnesium becausde high dose d3 over time can deplete a lot of magnesium which is used in the d3 activation process..So werite back top us on the knee situation thanks Jeff
There are so many brands of supplements available in health food stores and grocery stores. Have you any recommendations for either a source for the best Vitamen D or a reliable brand name to purchase? I know that supplements are not tested under the FDA, so I don’t want to be “scammed” by a junk supplement.
HI there
If you want to save a fortune on supplements get the bulk poweder instead of the pills. You will be set with 100% pure,
double tested vitamins and hormones at about a 90% discount to pills… you get the pure powder before the middlemen
put them into capsules and add
fake ingredients.. here is the info link for cheap pure powder supplier Peter at vitaspace.com >>>
https://jefftbowles.com/how-to-save-90percent-and-more-on-vitamins-hormones-supplements/
I love your book on Vitamin 3, Jeff, really fantastic. Increased my daily intake from 1000 I.U., to 5000 IU, now I’m up to 10,000. Feel really good except for constant urination, seems like I’m going like crazy every hour. I am also taking K2 & Magnesium. I’ve read the frequent urination can be a sign of toxicity? I’m wondering if I should cut back, or stop altogether.
Hi travis
Thanks for writing…
I have not heard of frequent urination as a problem before maybe you are getting normal urination now? I dont know..
the dose you are taking is similar to you sunbathing in the summer for a total of about 8 minutes!!!!
So I dont think toxicity is your problem.
Jeff. Thank you for your reply. I have googled the Dr’s protocol but it looks like I will need to contact one of those doctors about it because of concerns with calcium build up at high levels of d3 And maybe the use of magnesium
It’s confusing how much k2 to d3 is needed to control the calcium and what form/kind of d3 is best to take.
Currently I am trying Oralvisc. Have you heard of it
Your comments seem to say there is no need for k2 or mag because we take in a lot of d3 from the sun?
Hello there Debbie
Don’t waste your money on a doctor hypercalcemia is very rare happens to maybe 2 people in 1,000 and it is not really that dangerous..Resolves quickly when you stop the D3 . Just look for the warning signs
loss of appetite nausea rapid weight loss and this only happened to people after taking 300,000 to 600,00 a day for months with no K2 and who didnt know what symptoms to look for….
If you get nervous just ge a blood ca.ceiu, test in a few months…d3 itself is harmless…only the calcium released by bonew remodeling can be dangerous if it does not go back into your bones…this is so rare I would not worry about it…
keep in mind you make 20,000 iu of d3 in your skin by sunbathing in the summer for just 1/2 hour..You definitely should take magnesium. Save yourself some money just read my brand new ebook on the topic currently only 2.99!! it clears it all up and tells you why you need to take magnesium with d3 (0% of us are deficient in MG to being with. And why you might also want to add boron and zinc!
here is the link>>> https://www.amazon.com/dp/B07ZBP8QZZ
When i started taking 30,000 iu vitamin D3 (Solgar brand) per day, i started feeling amazing except for getting pain in the hips and ischial bursitis…anyone else have this response?
Hello there Meesh,
What might be going on is that you are remodeling old injuries or improperly remodeled tissues. The d3 activates the remodeling system to break down and rebuild these things in your body. IN the first book on d3 bad pains in the right hip and both shoulders wee described as lasting about 2 months and being quite painful. But after three moths the pains all went away…Some people say taking higher dose magnesium with the high dose d3 can prevent some of the pains.
Thanks very much for such wonderful reserch to best result or sure you serve humanity to your best. You should be rewarded dearly.
Why am I not getting these energizing effects from D3? I don’t really notice anything, actually. Fatigue, if anything. I take 60,000 IU/day along with 240 mcg K2 MK-7 and 1395 mg magnesium (750 from magnesium glycinate, 200 mg from magnesium citrate, and 445 mg from food). 651 mg calcium (200 mg from multivitamin and 451 mg from food).
Hello Joe
This fatigue you feel usually means that tyou are very low in mangeisum and the hgih dose D3 is eating up the low levels of magnesium in your body..
Faster than you can replace it withi supplements…u can only absorb a little magnesium each day..so ti takes time to build up your magnesium stores…
..My suggestion if I were you..I wold stop taking the d3 for a while and see if you can hadnle twice as much mangesoum but take it twice a day…the beter kind of magneisum to take is LEF’s extended release http://www.lef.org Take tyhis 2x a day for a week or two then try the d3 again….and start with a lower dose maybe 20,000 ius a day…whle yu stop the d3 still take the K2…as the d3 stays in your system a long time….but k2 does not
Vitamin D with K2 can apparently calcify a root canal. That happened to me. My dentist said she had never seen that happen before, except for once in a young person. I had been taking 10,000 IU D and about 16,000 IU K2 daily.
Someone needs to update the Wikipedia article on multiple sclerosis. It makes no mention of the Coimbra Protocol, and about vitamin D it states: ” Evidence suggests vitamin D supplementation, irrespective of the form and dose, provides no benefit for people with MS…”
wow that is really cool I will add that to the 1000+ high dose vitamin d3 case studies search engine!!! at JeffTbowles.com